Introduction
Airway management is a fundamental intervention in critically ill patients. Endotracheal intubation provides definitive airway protection and enables controlled oxygenation and ventilation, making it a cornerstone of anesthesiology, emergency medicine, and intensive care practice. Traditionally, difficult airway assessment has focused on anatomical factors such as limited mouth opening, restricted cervical spine mobility, and upper airway abnormalities that complicate glottic visualization and tube placement. Over the past decades, structured guidelines, particularly from the American Society of Anesthesiologists, have improved safety and standardized approaches for both anticipated and unanticipated difficult airways (1,2).
Despite these advances, tracheal intubation in critically ill patient´s remains associated with high morbidity and mortality. Many adverse events occur in patients with anatomically uncomplicated airways, often due to severe physiological disturbances present before intubation (3). Induction of anesthesia, transient apnea, and initiation of positive-pressure ventilation may exacerbate pre-existing respiratory, cardiovascular, or metabolic instability, potentially leading to profound hypoxemia, hypotension, or cardiac arrest.
Critically ill patients face a high risk of complications during intubation, even when their airway appears easy, due to their unstable physiological condition
Airway management in the intensive care unit (ICU) or emergency department differs substantially from controlled operating room environments. These patients frequently present with severe hypoxemia, circulatory compromise, or metabolic disturbances, reducing physiological reserve and increasing vulnerability to peri-intubation complications. Procedures are often performed under time constraints, with incomplete physiological stabilization, further heightening risk. Mosier introduced the concept of the physiologically difficult airway in 2015 to describe situations in which airway access may be technically straightforward, but the patient’s underlying physiological state places them at high risk for adverse outcomes during induction and initiation of mechanical ventilation (4). Recognition of this concept has expanded airway assessment beyond anatomy, emphasizing the importance of physiological optimization before, during, and after intubation.
Tracheal Intubation in Critically Ill Patients
Intubation outside the operating room carries substantially higher risk than elective procedures. Complications arise from both underlying disease and physiological effects of induction, apnea, and positive-pressure ventilation. The INTUBE study, a multicenter prospective cohort enrolling 2,964 critically ill adults from 197 sites across 29 countries, reported major adverse events in approximately 45% of patients within 30 minutes of intubation (5). Cardiovascular instability occurred in 42.6%, severe hypoxemia in 9.3%, and cardiac arrest in 3.1% (5). These findings highlight the importance of comprehensive physiological assessment and optimization prior to intubation.
Physiologically Difficult Airway in Critically Ill Patients
Critically ill patients have limited physiological reserve, reducing their ability to tolerate the stress associated with airway management. Induction of anesthesia results in suppression of sympathetic tone and spontaneous ventilation, while positive-pressure ventilation alters intrathoracic pressure and decreases venous return. In healthy individuals, these changes may be well tolerated, but in critically ill patients, they can rapidly precipitate hypoxemia, hypotension, or cardiovascular collapse (6). The physiologically difficult airway emphasizes that the main risks during tracheal intubation in this population are often due to underlying physiological instability rather than anatomical challenges alone.
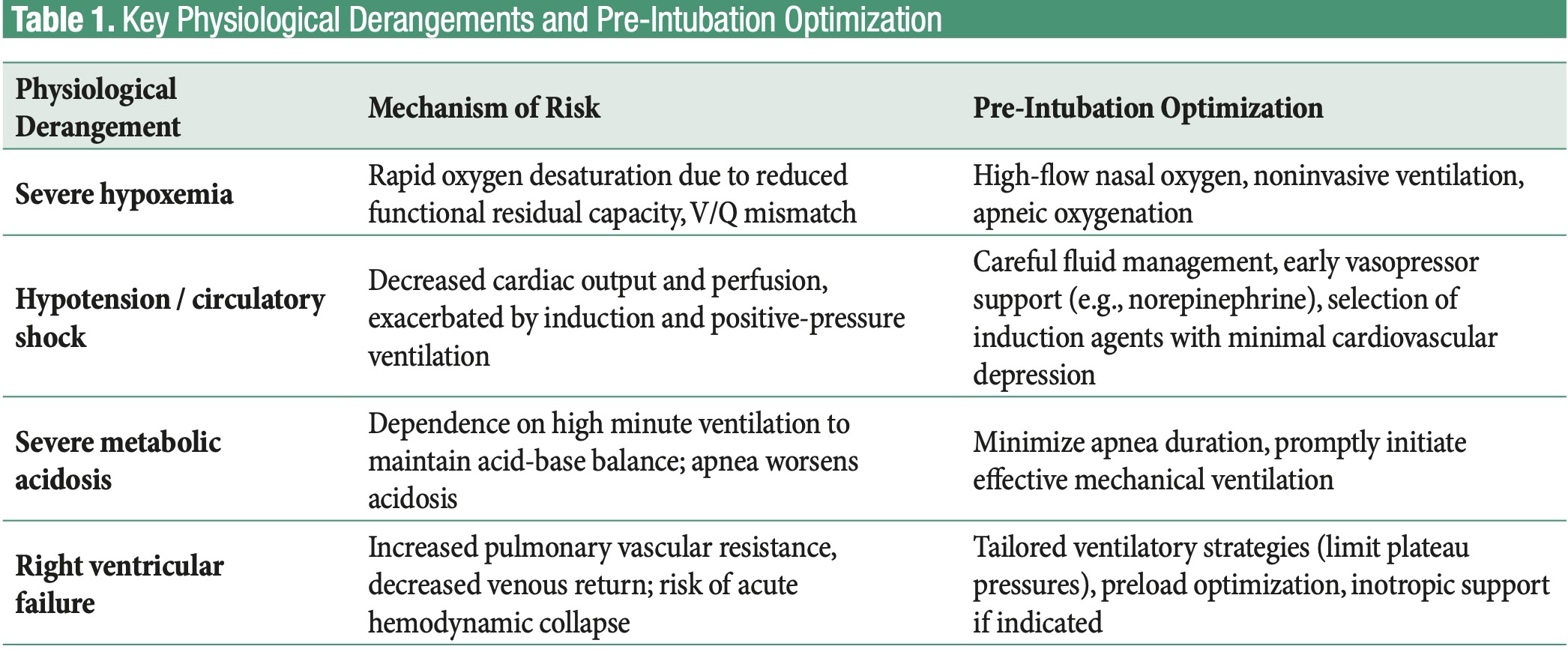
Four primary physiological derangements are associated with increased peri-intubation risk: severe hypoxemia, hypotension or circulatory shock, severe metabolic acidosis, and right ventricular failure. Other conditions, such as elevated intracranial pressure, obesity, or pregnancy, may further increase risk and should be considered during airway planning (6).
Severe hypoxemic respiratory failure dramatically shortens the safe apnea period. Patients with acute respiratory distress syndrome (ARDS), severe pneumonia, or pulmonary edema typically have reduced functional residual capacity and increased intrapulmonary shunting, which accelerate oxygen desaturation during apnea (7). Critically ill patients often have increased oxygen consumption and impaired gas exchange due to ventilation–perfusion mismatch. Even brief interruptions in ventilation during laryngoscopy may lead to critical hypoxemia. Preoxygenation strategies that go beyond standard oxygen delivery such as high-flow nasal oxygen (HFNO), non – invasive positive-pressure ventilation (NIV), or apnoeic oxygenation can improve oxygen stores, prolong safe apnoea time, and reduce peri-intubation hypoxemia (7).
Hemodynamic instability is another core factor. These patients frequently have compromised cardiovascular function due to sepsis, hemorrhage, or cardiogenic shock. Induction agents may decrease vascular tone and myocardial contractility, while positive-pressure ventilation further reduces venous return and cardiac output (7). This effect may be exacerbated by concurrent sedatives, vasodilators, or other medications. Optimization of hemodynamics before intubation, including fluid resuscitation when appropriate and early use of vasopressors such as norepinephrine, is essential. Selection of induction agents also impacts risk; ketamine and etomidate are often preferred over propofol due to their lesser cardiovascular depressive effects (8).
Severe metabolic acidosis presents unique challenges. Patients with diabetic ketoacidosis or lactic acidosis rely on high minute ventilation to maintain acid–base balance. Loss of spontaneous ventilation after induction can rapidly worsen acidosis, leading to hemodynamic instability, arrhythmias, or cardiac arrest. Minimizing apnea duration and promptly establishing adequate mechanical ventilation are critical in these patients.
Right ventricular failure further increases vulnerability. Positive-pressure ventilation raises pulmonary vascular resistance and reduces venous return, which can strain a right ventricle already functioning near maximal capacity, as in acute pulmonary embolism or chronic pulmonary hypertension. Even small increases in pulmonary pressures or reductions in preload may precipitate sudden hemodynamic collapse. Management may require tailored ventilatory strategies, careful fluid management, and inotropic support to preserve right ventricular function (8,9).
The main physiological risks during intubation in critically ill patients are severe hypoxemia, hypotension, metabolic acidosis, and right ventricular failure. Optimizing oxygenation, hemodynamics, and ventilation before intubation is essential to reduce complications.
Collectively, these physiological derangements underscore the complexity of airway management in critically ill patients. The main derangements and recommended pre-intubation optimization strategies are summarized in Table 1.
Management of the physiologically difficult airway
Successful management of the physiologically difficult airway requires a structured, physiologyfocused approach that anticipates and mitigates risks related to hypoxemia, hemodynamic instability, acid–base derangements, and right ventricular dysfunction. This strategy goes beyond securing anatomical access, emphasizing physiological optimization before, during, and after intubation, which improves outcomes and reduces periintubation complications (10,11).
Patient Assessment
Preparation begins with a comprehensive assessment of the patient’s physiological status and identification of highrisk features. Standardized airway management bundles that integrate patient assessment, oxygenation and hemodynamic optimization, airway equipment preparation, and planned postintubation monitoring have been associated with reduced rates of hypoxemia and other adverse events (11,12).
Oxygenation Strategies
Oxygenation optimization is a cornerstone of safe airway management. Preoxygenation aims to increase oxygen reserves
and prolong the duration of safe apnea. Traditional facemask oxygen delivery is often inadequate in critically ill patients due to poor alveolar recruitment and shunt physiology. Strategies such as noninvasive ventilation (NIV) or highflow nasal oxygen (HFNO) have been shown to improve oxygenation and reduce periintubation hypoxemia. For example, the PREOXI randomized trial found that preoxygenation with NIV significantly reduced the incidence of severe hypoxemia (SpO₂ <85%) compared with facemask oxygen (9.1% vs. 18.5%) among critically ill adults undergoing tracheal intubation (11). A recent systematic review and network metaanalysis supports the efficacy of NIV and HFNC over conventional oxygen therapy for reducing intubationassociated hypoxemia (13). These methods improve alveolar recruitment, increase functional residual capacity, and may allow continuous apneic oxygenation during laryngoscopy (8,13).
Safe airway management in critically ill patients requires anticipating and optimizing physiological risks, hypoxemia, hemodynamic instability, metabolic acidosis, and right ventricular dysfunction—beyond simply securing anatomical access.
Hemodynamic management
Hemodynamic support is critical. Periintubation hypotension and cardiovascular collapse are frequent and associated with poor outcomes. Proactive strategies include careful fluid management when appropriate and early preparation of vasopressor support. While evidence is not yet definitive on routine fluid boluses preventing hypotension, early initiation of vasopressors such as norepinephrine or phenylephrine remains common practice in unstable patients (13). Maintaining metabolic stability is essential, especially in patients with severe acidosis who depend on high minute ventilation to maintain acid–base balance. Minimizing apnea duration and rapidly achieving effective mechanical ventilation after intubation help prevent worsening acidosis and arrhythmias. Patients with right ventricular dysfunction require ventilatory strategies that avoid excessive increases in pulmonary vascular resistance. Tailored ventilator settings that limit plateau pressures and preserve venous return, along with preload optimization and inotropic support when indicated, can mitigate the risk of acute hemodynamic collapse (12).
First-pass intubation strategy
Procedural strategies that maximize firstpass intubation success reduce exposure to hypoxemia and hemodynamic instability. Evidence suggests that video laryngoscopy and adjuncts such as bougies increase firstpass success rates compared with direct laryngoscopy, particularly in highrisk settings, and should be considered when available (8,12,14). Multiple intubation attempts are associated with increased risk of desaturation, aspiration, and cardiovascular deterioration.
Structured strategies, including pre-intubation optimization, first-pass intubation techniques, and vigilant post-intubation monitoring, are essential to reduce peri-intubation complications and improve outcomes
Postintubation care is equally important. Continuous monitoring of oxygenation, ventilation, and hemodynamics allows early identification of deterioration. Implementation of lungprotective ventilation strategies, appropriate vasopressor titration, and correction of metabolic abnormalities reduce secondary complications. Structured airway bundles that include postintubation elements further enhance patient safety.
Conclusion
Airway management in critically ill patients is complicated not only by anatomical challenges but also by profound physiological instability. Severe hypoxemia, hemodynamic compromise, metabolic acidosis, and right ventricular failure substantially increase the risk of peri-intubation complications. Recognition of these high-risk physiological states, targeted pre-intubation optimization, structured procedural strategies, and vigilant post-intubation monitoring are essential for safe airway management. Integrating physiological considerations into airway planning enables clinicians to anticipate complications and tailor interventions, ultimately improving outcomes in critically ill patients.
Reference
- Apfelbaum JL, Hagberg CA, Caplan RA, Blitt CD, Connis RT, Nickinovich DG et al. American Society of Anesthesiologists Task Force on Management of the Difficult Airway. Practice guidelines for management of the difficult airway: an updated report by the American Society of Anesthesiologists Task Force on Management of the Difficult Airway. Anesthesiology. 2013;118(2):251-70. doi: 10.1097/ALN.0b013e31827773b2.
- Apfelbaum JL, Hagberg CA, Connis RT, Abdelmalak BB, Agarkar M, Dutton RP et al. 2022 American Society of Anesthesiologists Practice Guidelines for Management of the Difficult Airway. Anesthesiology. 2022;136(1):31-81. doi: 10.1097/ALN.0000000000004002.
- Mosier JM, Sakles JC, Law JA, Brown CA 3rd, Brindley PG. Tracheal Intubation in the Critically Ill.Where We Came from and Where We Should Go. Am J Respir Crit Care Med. 2020;201(7):775-788. doi: 10.1164/rccm.201908-1636CI.
- Mosier JM, Joshi R, Hypes C, Pacheco G, Valenzuela T, Sakles JC. The Physiologically Difficult Airway. West J Emerg Med. 2015;16(7):1109-17. doi: 10.5811/westjem.2015.8.27467.
- Russotto V, Myatra SN, Laffey JG, Tassistro E, Antolini L, Bauer P et al. INTUBE Study Investigators. Intubation Practices and Adverse Peri-intubation Events in Critically Ill Patients From 29 Countries. JAMA. 2021;325(12):1164-1172. doi: 10.1001/jama.2021.1727.
- Myatra SN, Divatia JV, Brewster DJ. The physiologically difficult airway: an emerging concept. Curr Opin Anaesthesiol. 2022;35(2):115-121. doi: 10.1097/ ACO.0000000000001102.
- Barbosa A, Mosier JM. Preoxygenation and apneic oxygenation in emergency airway management. Clin Exp Emerg Med. 2024;11(2):136-144. doi: 10.15441/ ceem.23.089.
- Jabaley CS. Managing the Physiologically Difficult Airway in Critically Ill Adults. Crit Care. 2023;27(1):91. doi: 10.1186/s13054-023-04371-3.
- Garcia SI, Smischney NJ, Sandefur BJ, D’Andria Ursoleo J, Kelm DJ,Wieruszewski PM. Peri-intubation Cardiovascular Collapse During Emergency Airway Management. Pulm Ther. 202511(4):569-585. doi: 10.1007/s41030-025-00326-x.
- Ren CE, Downing JV, Cardona S, Yardi I, Zahid M, Tang K et al. Impact of Interventions on Peri-Intubation Hypoxemia and Hypotension in Critically Ill Patients: Systematic Review and Meta-Analysis. West J Emerg Med. 2025;26(5):1380-1391. doi: 10.5811/westjem.41210.
- Gibbs KW, Ginde AA, Prekker ME, Seitz KP, Stempek SB, Taylor C et al. Protocol and statistical analysis plan for the PREOXI trial of preoxygenation with noninvasive ventilation vs oxygen mask. medRxiv. 2023:2023.03.23.23287539. doi: 10.1101/2023.03.23.23287539.
- Janz DR, Semler MW, Joffe AM, Casey JD, Lentz RJ, de Boisblanc BP et al. Check-UP Investigators*; Pragmatic Critical Care Research Group. A Multicenter Randomized Trial of a Checklist for Endotracheal Intubation of Critically Ill Adults. Chest. 2018;153(4):816-824. doi: 10.1016/j.chest.2017.08.1163
- Pitre T, Liu W, Zeraatkar D, Casey JD, Dionne JC, Gibbs KW et al. Preoxygenation strategies for intubation of patients who are critically ill: a systematic review and network meta-analysis of randomised trials. Lancet Respir Med. 2025;13(7):585-596. doi: 10.1016/S2213-2600(25)00029-3.
- Zhang K, Zhong C, Lou Y, Fan Y, Zhen N, Huang T et al.Video laryngoscopy may improve the intubation outcomes in critically ill patients: a systematic review and meta-analysis of randomised controlled trials. Emerg Med J. 2025;42(5):334-342. doi: 10.1136/emermed-2023-213860.
