Introduction
Psychogenic non-epileptic seizures (PNES), also known as functional seizures, are episodic events that clinically resemble epileptic seizures but occur without ictal epileptiform activity (1). They fall within the spectrum of functional neurological disorders (FND) and are driven by psychological mechanisms rather than abnormal cortical discharges. PNES account for a substantial proportion of seizure-related ED visits and frequently lead to unnecessary pharmacologic interventions. Emergency clinicians are often the first providers to evaluate acute seizure-like presentations. Given time pressures and the potential for catastrophic consequences of missed convulsive status epilepticus, PNES is both easily overlooked and often over-treated (2,3). Recognition of PNES in the ED is critical for preventing iatrogenic complications and ensuring appropriate follow-up.
Epidemiology and pathophysiology
PNES are estimated to affect 2–33 per 100,000 individuals, though true prevalence may be higher due to under-recognition. Among all patients referred to epilepsy centers, 10–40% is ultimately diagnosed with PNES. In emergency settings, studies suggest that up to one-third of patients treated for status epilepticus may in fact be experiencing PNES episodes. PNES is more common in women (approximately 70% of cases) and frequently arises during adolescence or early adulthood (4). Risk factors include trauma, chronic psychological stress, psychiatric comorbidities (e.g., depression, anxiety, PTSD), and a history of chronic pain or somatization. The pathophysiology of PNES is conceptualized within modern frameworks of functional neurological disorders, where alterations in attention, emotion regulation, and sensorimotor processing create involuntary symptoms without structural neurological disease (5).
PNES are common seizure-like events in the ED, driven by psychological mechanisms, and early recognition is essential to prevent unnecessary interventions and iatrogenic harm.
Clinical presentation
PNES (psychogenic nonepileptic seizures) can mimic virtually any seizure semiology; however, several clinical characteristics increase suspicion for this diagnosis, particularly in the emergency department. Compared with typical epileptic generalized tonic-clonic seizures, PNES episodes are often of longer duration, usually exceeding 2–3 minutes, and are characterized by a gradual onset and offset rather than abrupt transitions (table 1). Motor manifestations commonly include asynchronous or side-to-side movements, pelvic thrusting, irregular thrashing, head rolling, and other non-stereotyped movement patterns that may vary between events. Eye closure during the episode is frequent and may be accompanied by resistance to passive eye opening. Protective reflexes are typically preserved, including avoidance of injury during falls. Ictal crying, verbalization, or prominent emotional expression may occur. After the event, post-ictal confusion is usually absent or very brief. Autonomic signs are generally minimal, with limited tachycardia, cyanosis, hypersalivation, or tongue biting.
In contrast, although no single feature is definitive, findings that are less consistent with PNES and raise concern for epileptic seizures include lateral tongue biting, highly stereotyped tonic-clonic activity, post-ictal confusion lasting longer than 5–10 minutes, documented medication non-adherence in patients with known epilepsy, and witnessed apnea or cyanosis (6).
PNES mimic epileptic seizures, but prolonged, non-stereotyped episodes with preserved reflexes and minimal post-ictal confusion suggest PNES.
Features less consistent with psychogenic nonepileptic seizures
In contrast, although no single feature is definitive, findings that are less consistent with PNES and raise concern for epileptic seizures include lateral tongue biting, highly stereotyped tonic-clonic activity, post-ictal confusion lasting longer than 5–10 minutes, documented medication non-adherence in patients with known epilepsy, and witnessed apnea or cyanosis. Ultimately, definitive differentiation between PNES and epileptic seizures often requires further evaluation, with video-EEG monitoring considered the diagnostic gold standard (7).
Diagnostic evaluation in the emergency department
Initial priorities
Emergency clinicians must prioritize stabilization, treating life-threatening conditions first. The guiding principle is: PNES can only be diagnosed after ruling out acute medical emergencies, including epileptic seizures, hypoglycemia, electrolyte derangements, toxicologic causes, and trauma (8).
Bedside assessment
Bedside assessment of a suspected PNES episode should include several key components. Vital signs should be measured, noting that PNES often lack pronounced autonomic changes. A focused neurologic examination should be performed both before and after the event. Bedside glucose testing is important to exclude metabolic causes of altered consciousness or seizure-like activity. Gathering a detailed history from witnesses is crucial, emphasizing the onset, duration, movement patterns, and the patient’s state after the event. Finally, reviewing the patient’s prior diagnoses, psychiatric history, and current medications helps provide context and may assist in differentiating PNES from epileptic seizures.
Key components of bedside assessment for suspected PNES include measurement of vital signs, noting that PNES often lack pronounced autonomic changes; performing a focused neurologic examination before and after the event; bedside glucose testing to exclude metabolic causes; obtaining a detailed history from witnesses, with emphasis on onset, duration, movement patterns, and the patient’s post-event state; and reviewing prior diagnoses, psychiatric history, and current medications (2,8,9).
Laboratory and imaging testing
Routine laboratory evaluation may include electrolytes, pregnancy testing, and toxicology screens when clinically indicated. Neuroimaging is not mandatory unless trauma, focal deficits, or first-time seizure concerns are present.
Role of electroencephalography
Gold standard diagnosis requires event capture during video-EEG monitoring, which is rarely available in the ED. Short-term ED EEG may help exclude ongoing epileptic activity in suspected status epilepticus.Normal interictal EEG does not confirm PNES and should not be used diagnostically.
Bedside maneuvers
Gentle verbal reassurance and instructions (e.g., asking patient to open eyes or follow simple commands) may differentiate PNES from epileptic seizures in some cases. These must be used ethically and never confrontationally (10).
Management in the emergency department
Table 2 shows the recommended emergency department workup for suspected psychogenic nonepileptic seizures.
General principles
Once life-threatening conditions have been excluded and PNES is suspected, it is important to avoid escalating antiepileptic medications or sedatives, as these provide no benefit and may increase the risk of respiratory depression. Supportive monitoring should be maintained until the episode resolves. Additionally, any comorbid conditions, such as anxiety or metabolic abnormalities, should be identified and treated appropriately.
Communication with the patient
Clear, compassionate communication is essential when managing suspected PNES. Patients should be reassured that their symptoms are real and involuntary. Clinicians should avoid statements such as “nothing is wrong” or any implication that the events are intentional. It is helpful to briefly explain that the episodes may represent a functional neurological disorder, which requires outpatient evaluation. Patients should be encouraged to follow up with neurology or specialized Functional Neurological Disorder / Psychogenic Nonepileptic Seizures services for further management (FND/PNES) (11).
Avoiding iatrogenic harm in patients with suspected psychogenic nonepileptic seizures
In patients with suspected PNES, common unnecessary interventions include repeated boluses of benzodiazepines or antiseizure medications, intubation for non-epileptic “status epilepticus,” and excessive imaging or laboratory testing. Studies have demonstrated that inappropriate intubation and ICU admission carry substantial risks, including complications related to sedation, mechanical ventilation, and prolonged hospitalization, without providing clinical benefit (table 3).
Management of suspected PNES in the ED focuses on avoiding unnecessary interventions, providing supportive care, clear patient communication, and ensuring safe disposition with appropriate outpatient follow-up.
Disposition Planning
After stabilization, appropriate disposition decisions for patients with suspected PNES include safe discharge with clear instructions and outpatient follow-up when events strongly suggest PNES and there is no medical instability. Neurology consultation should be obtained if the diagnosis remains uncertain. Psychiatric evaluation is indicated when there is acute behavioral risk, suicidality, or severe emotional distress (12,13).
Long-term management
Although long-term management generally falls outside the emergency department’s scope, awareness of evidence-based interventions can help guide disposition and follow-up planning. Recommended interventions include cognitive behavioral therapy (CBT), trauma-focused therapies when post-traumatic stress disorder (PTSD) is present, and multidisciplinary programs for functional neurological disorders. Comorbid psychiatric conditions, such as anxiety or depression, should be addressed, and patients should receive education about seizure physiology and stress responses. Anti-seizure medications are not effective for PNES unless coexisting epilepsy is confirmed (14).
Special populations
Children and Adolescents
PNES may present differently in younger patients and often relate to school stress, bullying, family dysfunction, or trauma. In the ED, evaluation should include careful psychosocial assessment and parental guidance (15).
Older Adults
PNES is less common but may be misinterpreted as late-onset epilepsy or syncope. Comorbid cognitive decline can complicate diagnosis.
Coexisting Epilepsy
Up to 10–20% of patients with PNES also have epileptic seizures. Lack of clear differentiation in the ED necessitates caution; follow-up EEG monitoring is essential.
Implications for emergency medicine practice
Enhancing recognition of PNES in the emergency department can reduce unnecessary use of antiepileptic medications and decrease iatrogenic complications, including respiratory depression and ICU admission. Improved recognition may also shorten ED length of stay, optimize resource utilization, and enhance patient trust while facilitating appropriate referral pathways. Educational initiatives, such as simulation training, standardized care pathways, and recognition checklists, and adherence to diagnostic algorithms (fig 1), have been shown to improve clinician comfort and diagnostic accuracy (12).
Rapid recognition of PNES in the ED, coupled with avoidance of unnecessary interventions, empathetic communication, and structured referral pathways, reduces harm and improves patient outcomes.
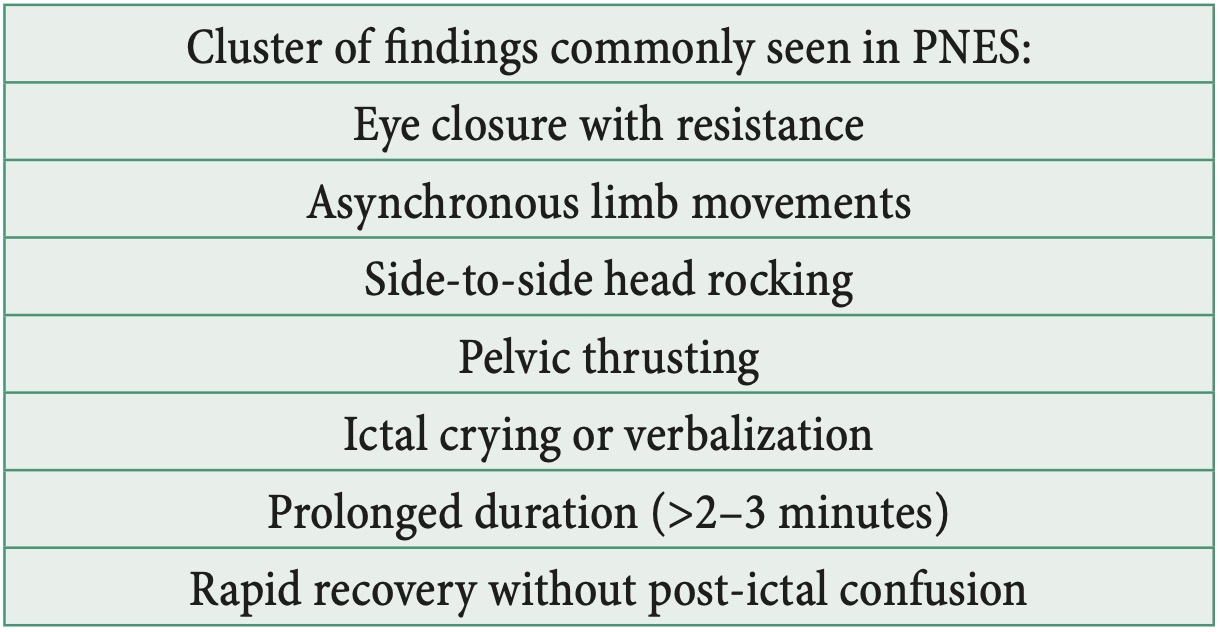
Figure 2. Clinical Signs Supporting PNES Diagnosis
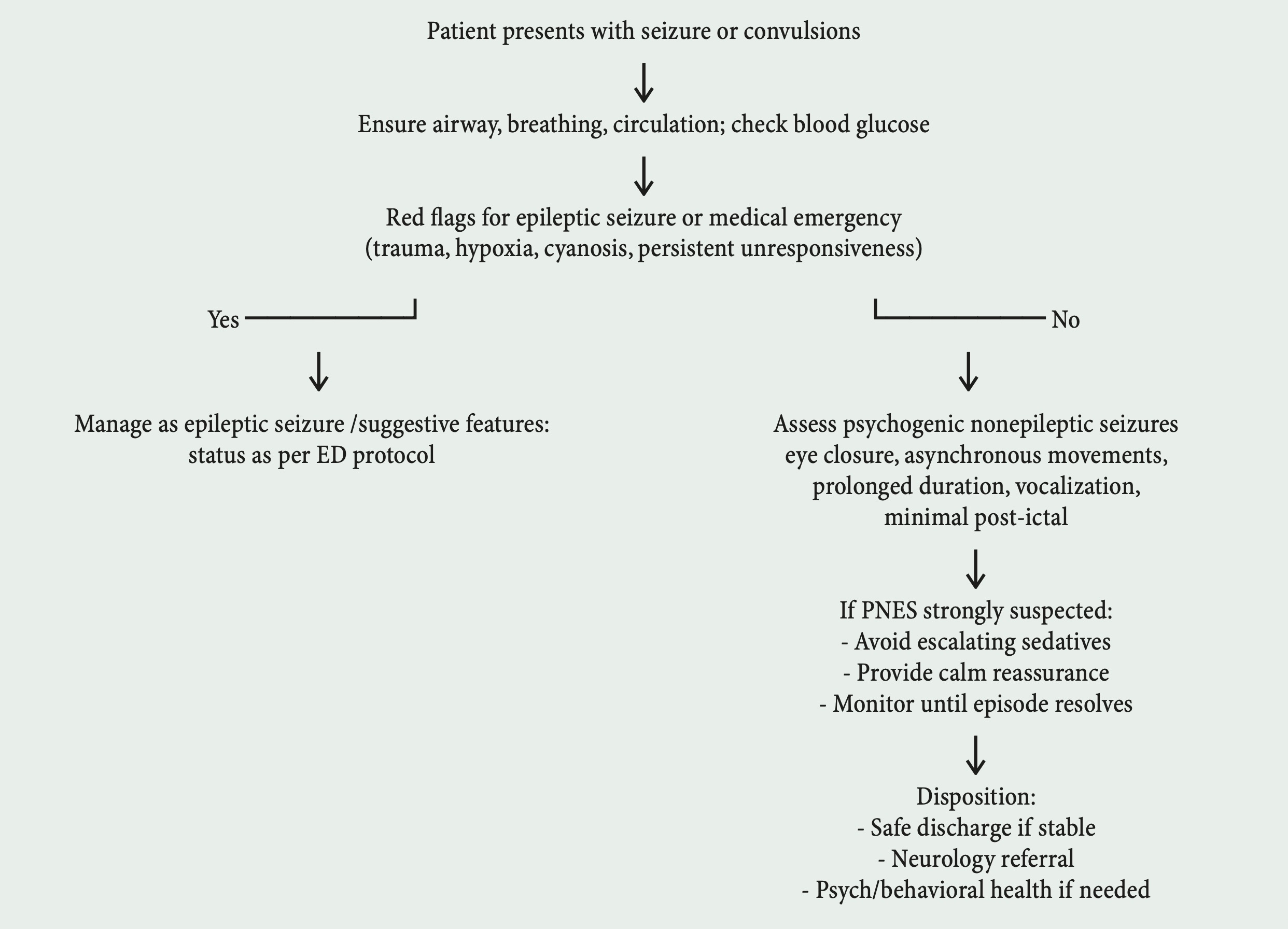
Figure 1. Practical emergency department algorithm for suspected psychogenic nonepileptic seizures
Conclusion
Psychogenic non-epileptic seizures are a frequent and challenging presentation in the emergency department. Effective ED management hinges on rapid identification of features suggestive of PNES, avoidance of unnecessary interventions, empathetic communication, and appropriate referral for definitive diagnosis and long-term care. Greater clinician awareness and structured management approaches can significantly reduce harm and improve outcomes for this vulnerable population.
References
-
Reuber M, Rawlings GH. Handbook of Clinical Neurology. Nonepileptic seizures – subjective phenomena.
Vol 139. 2016; p. 283–296. doi:10.1016/B978-0-12-801772-2.00025-4.
-
Alessi N, Perruca P, McIntosh AM. Missed, mistaken, stalled: Identifying components of delay to diagnosis in epilepsy.
Epilepsia. 2021;62(7):1494–1504. doi:10.1111/epi.16929.
-
Anzellotti F, Dono F, Evangelista G, Di Pietro M, Carrarini C, Russo M et al.
Psychogenic Non-epileptic Seizures and Pseudo-Refractory Epilepsy, a Management Challenge.
Front Neurol. 2020;11(461):1–14. doi:10.3389/fneur.2020.00461.
-
Asadi-Pooya AA, Sperling MR. Epidemiology of psychogenic nonepileptic seizures.
Epilepsy Behav. 2015;46:60–65. doi:10.1016/j.yebeh.2015.03.015.
-
Tojek TM, Lumley M, Barkley G, Mahr G, Thomas A.
Stress and Other Psychosocial Characteristics of Patients With Psychogenic Nonepileptic Seizures.
Psychosomatics. 2020;41(3):221–226. doi:10.1176/appi.psy.41.3.221.
-
Duncan R, Oto M. Predictors of antecedent factors in psychogenic nonepileptic attacks: multivariate analysis.
Neurology. 2008 Sep 23;71(13):1000–1005. doi:10.1212/01.wnl.0000326593.50863.21.
-
Muthusamy S, Ding C, Phan TG. Using Semiology to Classify Epileptic Seizures vs Psychogenic Nonepileptic Seizures:
A Meta-analysis. Neurol Clinic Pract. 2022 Jun;12(3):234–247.
doi:10.1212/CPJ.0000000000001170.
-
Reuber M. Psychogenic nonepileptic seizures: answers and questions.
Epilepsy Behav. 2008 May;12(4):622–635. doi:10.1016/j.yebeh.2007.11.006.
Epub 2007 Dec 27. PMID:18164250.
-
LaFrance WC Jr, Baker GA, Duncan R, Goldstein LH, Reuber M.
Minimum requirements for the diagnosis of psychogenic nonepileptic seizures: a staged approach.
Epilepsia. 2013 Nov;54(11):2005–2018. doi:10.1111/epi.12356.
-
Avbersek A, Sisodiya S. Does the primary literature provide support for clinical signs used to distinguish
psychogenic nonepileptic seizures from epileptic seizures?
J Neurol Neurosurg Psychiatry. 2010;81(7):719–725. doi:10.1136/jnnp.2009.197996.
-
Kanemoto K, LaFrance WC Jr, Duncan R, Gigineishvili D, Park SP, Tadokoro Y et al.
PNES around the world: Where we are now and how we can close the diagnosis and treatment gaps.
Epilepsia Open. 2017 Jun 23;2(3):307–316. doi:10.1002/epi4.12060.
Erratum in: Epilepsia Open. 2019 Jan 07;4(1):219. doi:10.1002/epi4.12291.
-
LaFrance WC Jr, Baird GL, Barry JJ, Blum AS, Frank Webb A, Keitner GI et al.
NES Treatment Trial (NEST-T) Consortium. Multicenter pilot treatment trial for psychogenic nonepileptic seizures:
a randomized clinical trial. JAMA Psychiatry. 2014 Sep;71(9):997–1005.
doi:10.1001/jamapsychiatry.2014.817.
-
Kerr MP, Mensah S, Besag F, de Toffol B, Ettinger A, Kanemoto K et al.
International League of Epilepsy (ILAE) Commission on the Neuropsychiatric Aspects of Epilepsy.
Epilepsia. 2011 Nov;52(11):2133–2138. doi:10.1111/j.1528-1167.2011.03276.x.
-
Dworetzky BA, Mortati KA, Rossetti AO, Vaccaro B, Nelson A, Bromfield EB.
Clinical characteristics of psychogenic nonepileptic seizure status in the long-term monitoring unit.
Epilepsy Behav. 2006 Sep;9(2):335–338. doi:10.1016/j.yebeh.2006.06.007.
-
Zhang LP, Jia Y, Huang H, Li DW, Wang YP.
Clinical Classifications of Children With Psychogenic Non-epileptic Seizure.
Front Pediatr. 2020;8:596781. doi:10.3389/fped.2020.596781.
