Introduction
Acute dyspnea is one of the the most common and urgent reasons for emergency department (ED) visits and is frequently caused by acute heart failure (AHF). Other causes usually are pneumonia, pulmonary embolism, or chronic obstructive pulmonary disease (1). Rapid and accurate differentiation of these conditions is critical to initiating appropriate therapy and improving patient outcomes (2). Chest radiography (CXR) is mostly used tool in the evaluation of acute dyspnea. CXR, due to its broad availability, is typically the first imaging modality utilized. However, its sensitivity in early cardiogenic pulmonary edema is limited, and interpretation may be delayed, particularly in busy ED settings (3). Lung ultrasound (LUS) has emerged as a rapid, bedside, radiation-free, non-invasive technique that detects extravascular lung water through identification of B-lines (4,5). LUS is easily repeatable, requires minimal equipment, and can be performed in real time during initial patient assessment. Most diagnostic accuracy studies for AHF use a composite reference standard combining clinical, laboratory, and imaging data, often supplemented by echocardiography, to minimize bias and provide a robust benchmark (6).
Lung ultrasound enables rapid, non-invasive bedside diagnosis of acute heart failure, significantly faster than chest X-ray in acute dyspnea patients.
We hypothesised that lung ultrasound in patients with acute dyspnea has at least equal diagnostic value compared to CXR and that is significantly faster in the emergency setting.
Therefore, the aim of this study was to compare the diagnostic performance of lung ultrasound with that of chest X-ray in patients presenting with acute dyspnea in the emergency department.We evaluated the time required for each diagnostic method and to determine whether LUS can accelerate diagnostic decisionmaking while maintaining comparable accuracy. We we like to make LUS a valuable first-line tool in the emergency evaluation of acute dyspnea.
Methods
Participants
This study was conducted at the Emergency Department of the University Hospital Centre Zagreb and enrolled 242 adult patients (>18 years) presenting with acute dyspnea of ≤3 days’ duration in which AHF was considered a differential diagnosis. Eligible patients were conscious, spontaneously breathing, and did not require mechanical ventilation.Written informed consent was obtained. Exclusion criteria included unconsciousness, need for invasive or non-invasive ventilation, hemodynamic instability requiring immediate intervention, current dialysis, chest trauma, or refusal to participate.
Data collection and clinical assessment
After confirming eligibility and consent, patients underwent a standardized diagnostic protocol including clinical examination, chest X-ray (CXR), and lung ultrasound (LUS). Final diagnosis was established by expert clinicians using all clinical data excluding knowledge of LUS results and served as the reference standard.
Chest X-ray
CXR was performed in posteroanterior and lateral views. Images were interpreted by board-certified radiologists who were blinded to the LUS results. Radiologic criteria for AHF included pulmonary venous redistribution, Kerley B lines, and interstitial or alveolar oedema. The presence of any of these signs classified the CXR as positive.
Lung ultrasound
Lung ultrasound was performed immediately after examination with patients in a supine or sitting position depending on clinical status. Two ultrasound machines were used: Esaote My Lab Six CrystaLine (1–8 MHz convex probe) and Philips Affiniti 70 (1–5 MHz convex probe). Scanning followed the international BLUE protocol, examining eight chest zones (bilateral anterior upper/lower and lateral upper/ basal areas). A diagnosis of AHF by LUS required ≥2 positive regions bilaterally with ≥3 B-lines per region. Initial operator was the principal investigator, with a second blinded examiner rescanning in unclear cases.
Statistical analysis
Quantitative data (examination times) were expressed as medians and quartile ranges. Examination times were recorded and compared between LUS and CXR. Statistical significance was set at p<0.05. Sample size requirements were calculated using an online calculator provided by Akoglu (7).
Results
The median age was 79 years (range 30–100). Females were more frequently admitted (133 females, median age 80; 109 males, median age 76). Median ages were similar in patients with (80 years) and without AHF (77 years).
The time to ultrasound findings showed a relatively narrow distribution, ranging from 4.0 to 75.0 minutes, with a median of 10.0 minutes and a quartile range from 8.0 to 14.0 minutes. The median waiting time for chest X-ray results was 62.5 (28.25-106.5) minutes, with the longest waiting time recorded at 474.0 minutes. All LUS results preceded CXR reports (Table 1) (Figure 1).
Discussion
Key strength of LUS is its rapid availability. The main finding of our study is that LUS the time to results was significantly shorter than for CXR (median 10.0 vs. 62.5 minutes), supporting its role as a first-line test in acute dyspnea. The clinical importance of speed should not be underestimated.
Desctiptive parameter (min)
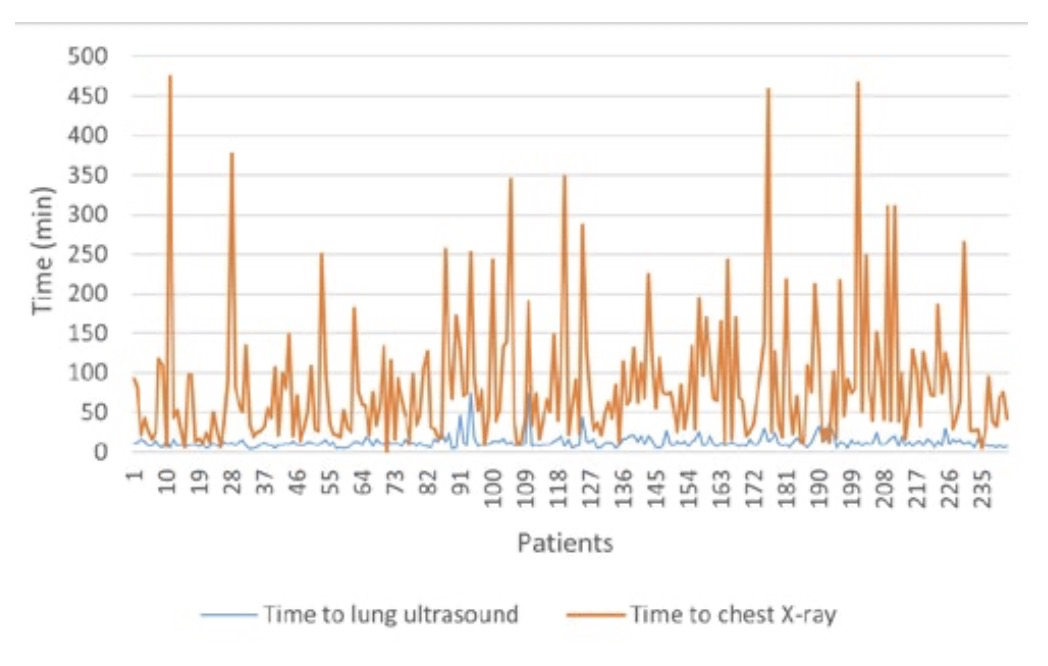
Figure 1. Time to lung ultrasound and chest radiography
Rapid diagnosis facilitates the initiation of earlier treatment, which may improve outcomes. For example, point-of-care LUS has been shown to alter diagnoses in a substantial proportion of patients, directly influencing management decisions (8). Moreover, studies report that LUS use improves patient flow and resource utilisation in emergency departments (9), reduces delays in critical care linked to higher mortality (10), and contributes to shorter length of stay and better survival outcomes (11). Together, these findings suggest that, beyond diagnostic accuracy, the timeliness of LUS may have significant downstream effects on both patient care and healthcare efficiency.
Faster lung ultrasound diagnosis supports early detection of acute heart failure and timely initiation of treatment in the emergency department.
Overall, while LUS cannot replace more specific modalities for confirming AHF, it offers an ideal balance of high sensitivity and rapid availability. In the emergency department, where rapid triage and exclusion of life-threatening conditions are paramount, LUS is best applied as a front-line rule-out tool integrated with confirmatory tests for comprehensive evaluation.
Conclusion
Lung ultrasound demonstrated significantly shorter time to results and faster diagnosis.
These findings support its use as a rapid, non-invasive, first-line tool for excluding acute heart failure in acute dyspnoic patients.
Acknowledgement
The authors would like to express their gratitude to all participants, their families, and the colleagues who contributed to participant recruitment.
Reference
- Zoorob RJ, Campbell JS. Acute dyspnea in the office. Am Fam Physician. 2003;68(9):1803-10. PMID: 14620600.
- Santus P, Radovanovic D, Saad M, Zilianti C, Coppola S, Chiumello DA et al. Acute dyspnea in the emergency department: a clinical review. Intern Emerg Med. 2023;18(5):1491-1507. doi: 10.1007/s11739-023-03322-8.
- Cardinale L, Volpicelli G, Lamorte A, Martino J, Andrea Veltri. Revisiting signs, strengths and weaknesses of Standard Chest Radiography in patients of Acute Dyspnea in the Emergency Department. J Thorac Dis. 2012;4(4):398-407. doi: 10.3978/j.issn.2072-1439.2012.05.05.
- Haaksma ME, Smit JM, Heldeweg MLA, Pisani L, Elbers P, Tuinman PR. Lung ultrasound and B-lines: B careful! Intensive Care Med. 2020;46(3):544-545. doi: 10.1007/s00134-019-05911-8.
- Gargani L. Lung ultrasound: a new tool for the cardiologist. Cardiovasc Ultrasound. 2011;9:6. doi: 10.1186/1476-7120-9-6.
- Martindale JL, Wakai A, Collins SP, Levy PD, Diercks D, Hiestand BC et al. Diagnosing Acute Heart Failure in the Emergency Department: A Systematic Review and Meta-analysis. Acad Emerg Med. 2016;23(3):223-42. doi: 10.1111/ acem.12878.
- Akoglu H. User’s guide to sample size estimation in diagnostic accuracy studies. Turk J Emerg Med. 2022;22(4):177-185. doi: 10.4103/2452-2473.357348.
- Heldeweg MLA, Vermue L, Kant M, Brouwer M, Girbes ARJ, Haaksma ME et al. The impact of lung ultrasound on clinical-decision making across departments: a systematic review. Ultrasound J. 2022;14(1):5. doi: 10.1186/s13089-021-00253-3.
- Ciumanghel I, Barbuta E, Ciumanghel AI, Buzincu I, Grigorasi G, Cimpoesu D. Point-of-care lung ultrasound – a rapid and reliable diagnostic tool for emergency physicians treating patients with acute dyspnea in high-volume emergency departments. Emerg Radiol. 2025;32(3):329-338. doi: 10.1007/s10140-025-02343-4.
- Groenland CNL, Termorshuizen F, Rietdijk WJR, van den Brule J, Dongelmans DA, de Jonge E et al. Emergency Department to ICU Time Is Associated With Hospital Mortality: A Registry Analysis of 14,788 Patients From Six University Hospitals in The Netherlands. Crit Care Med. 2019;47(11):1564-1571. doi: 10.1097/CCM.0000000000003957.
- Baloescu C, Parhar A, Liu R,Wanjiku GW. Effect of Point-of-Care Ultrasound on Clinical Outcomes in Low-Resource Settings: A Systematic Review. Ultrasound Med Biol. 2022;48(9):1711-1719. doi: 10.1016/j.ultrasmedbio.2022.04.221.
