Introduction
The chain of care for emergency patients in Croatia consists of ground emergency medical service (GEMS) teams, unified emergency admissions, and recently, helicopter emergency medical service (HEMS) teams.HEMS in Croatia was established in April 2024 and operates in four bases: the Rijeka and Split bases are operational 24 hours a day and the Osijek and Zagreb bases are operational during daylight hours. Interventions to which the HEMS team is assigned can be primary, secondary or interhospital transports. The HEMS team can be dispatched directly to the scene of the intervention immediately after receiving the call and such interventions are called primary. In secondary interventions, the helicopter service team is dispatched to the agreed meeting point with the GEMS team (1).
The Zagreb base covers the area of nine surrounding counties, which is home to almost half of the population of Croatia (2). The hospital system in Croatia is organized at the regional and national levels. Regional hospitals provide secondary-level healthcare and, by their very organizational structure, do not have all medical and diagnostic services, and are therefore not able to provide definitive care for certain categories of patients, such as polytraumatized patients, patients with cerebrovascular incident or myocardial infarction. National hospitals have such an opportunity.
The Croatian network of primary percutaneous coronary intervention is organized according to regional centers covering certain areas, meaning that the patients who require such intervention are not always transported to the nearest hospital. The treatment of cerebrovascular incidents depends on local protocols, which mostly include initial treatment and thrombolysis in the nearest facility that can provide it. However, the latest guidelines for stroke treatment recommend direct transport to a facility capable of performing endovascular thrombectomy, especially if there is no possibility of rapid subsequent interhospital transport (less than 45 minutes) (3).
In many countries, the guidelines for injured patient care increasingly emphasize rapid transport to an appropriate facility that can provide definitive care for the patient’s life-threatening injuries. This is precisely why it is important to develop thrombectomy centers and thus ensure patient care (4,5,6).
Numerous studies have been conducted on the effectiveness and cost-effectiveness of helicopter emergency services, and most note that it is difficult to draw definitive conclusions due to data heterogeneity.
Evidence on the effectiveness and cost-effectiveness of helicopter emergency services remains inconclusive due to variability in study data.
The key conclusion is that early arrival at an appropriate facility improves better outcomes and quality of life. However, HEMS is not necessarily always faster. Studies by individual countries on the cost-effectiveness of emergency helicopter service depending on the distance from the appropriate facility have shown that HEMS has an advantage over GEMS if the distance is greater than 50 km (7,8). The aim of this study was to compare time to scene/patient and transport time between HEMS and GEMS in primary activations of the Zagreb HEMS base during 2025.
Methods
This retrospective study includes all patients for whose care the emergency helicopter service of the Zagreb base was primarily activated between January 1, 2025 and December 21, 2025. General patient data, medical intervention criteria, and flight data were obtained from medical and flight records from the “e-hitna” program. The HEMS team time to scene includes activation time and flight time to the intervention site. The activation time must not exceed 5 minutes, but can sometimes be longer due to specific circumstances. Ideal approach for GEMS would be to determine EMS team response times using official EMS operational data but we were not able to use it.
Therefore, times related to the GEMS team were estimated using Google Maps in an ideal time period without traffic congestion. It is assumed that the team to arrive at the intervention site is the one whose base is closest, regardless of whether it is a team with a doctor or with two nurses.
All patients, except children, were transported by helicopter service to the same clinical hospital. It was assumed that GEMS teams would transport these patients to tertiary centers in Zagreb according to existing protocols if the definitive care for their condition was not available in the corresponding institution. Statistical analysis was performed using Microsoft Excel. Quantitative data were expressed as medians.
Results
During 2025, the Zagreb HEMS base was activated a total of 398 times, of which 111 were primary interventions, meaning that the helicopter team was activated and sent to the scene of the incident immediately after the intervention was reported.
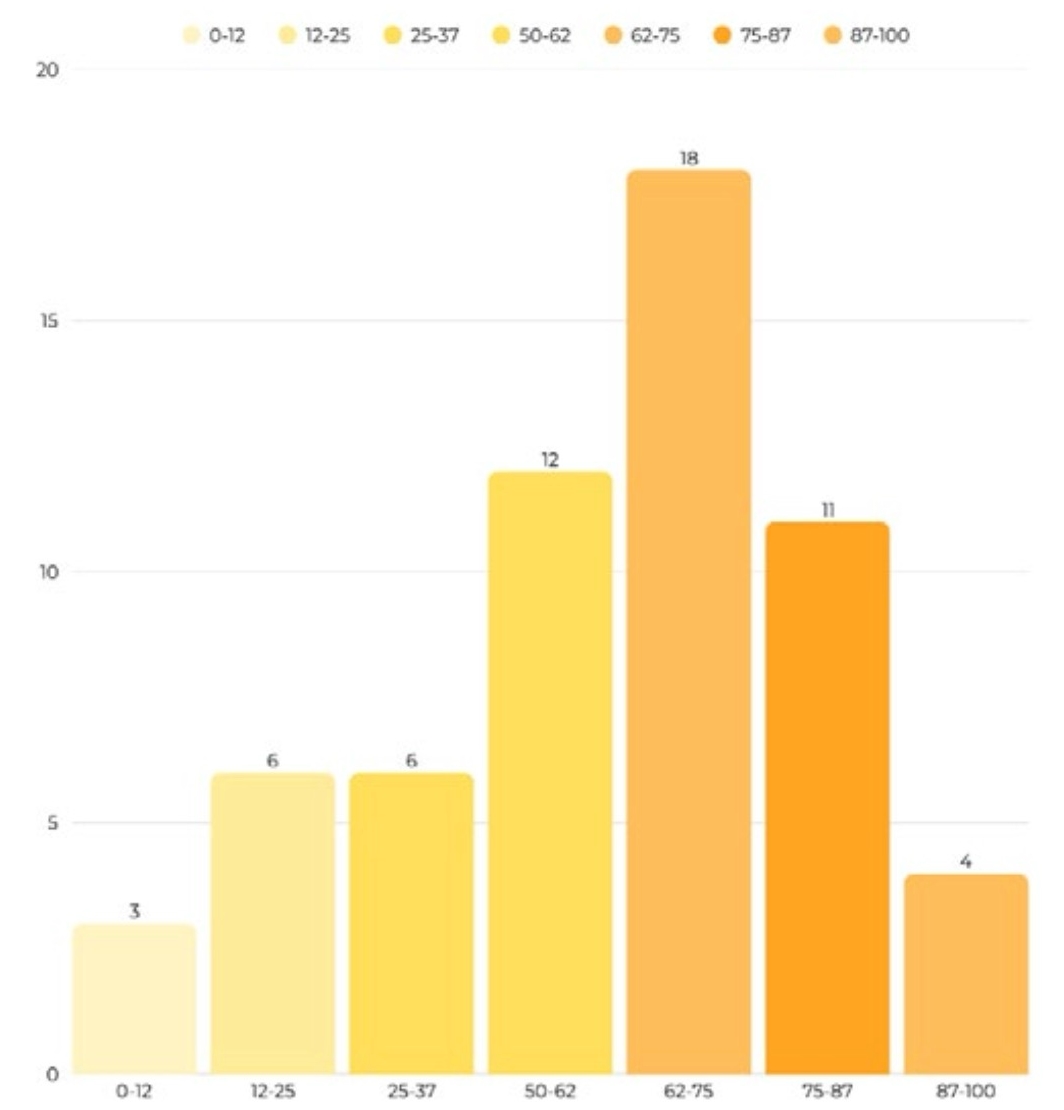
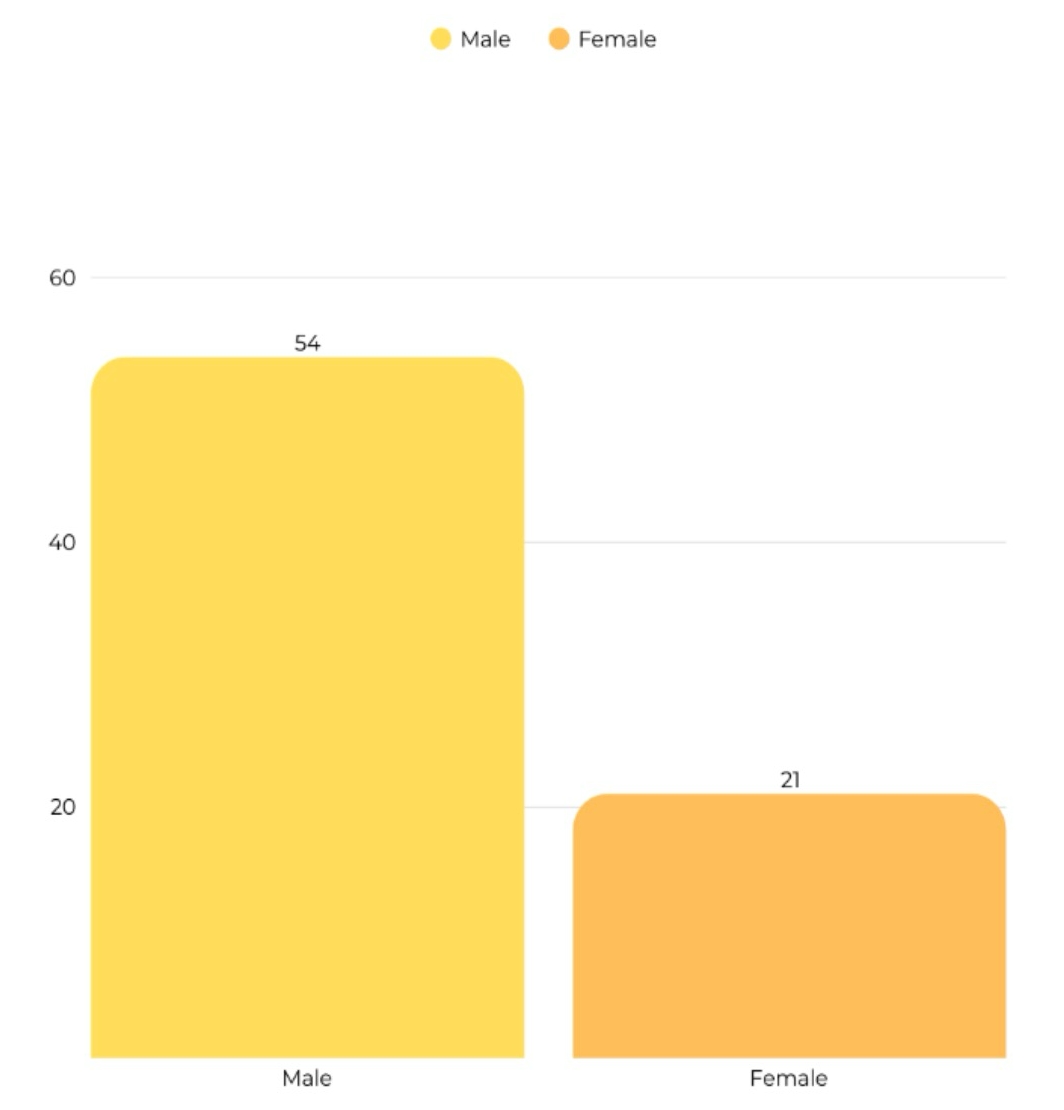
A total of 75 patients were treated at tertiary centers. The remaining patients, out of a total of 111, were not treated in a tertiary center for several reasons. Most commonly, this was because the intervention was discontinued, patient died, or the patient was managed at another healthcare facility and did not require treatment in a tertiary center.The median age was 59,with the exception of two patients for whom data was not available (Figure 1). The majority were men, 54 of them (Figure 2).
The helicopter team was most often dispatched to traffic accidents and other injuries, as many as 48 times. It was activated 16 times due to suspected neurological events, and 9 times due to internal medicine emergencies, most often due to suspected acute coronary syndrome. The team was dispatched twice to treat a patient with choking due to a foreign body airway obstruction.
The HEMS team had a shorter time to the scene of the intervention in 43 cases, the GEMS team in 31 cases, and arrival times were equal in one case. The median difference in time to scene between helicopter and ground teams was 3 minutes in favor of the helicopter team.
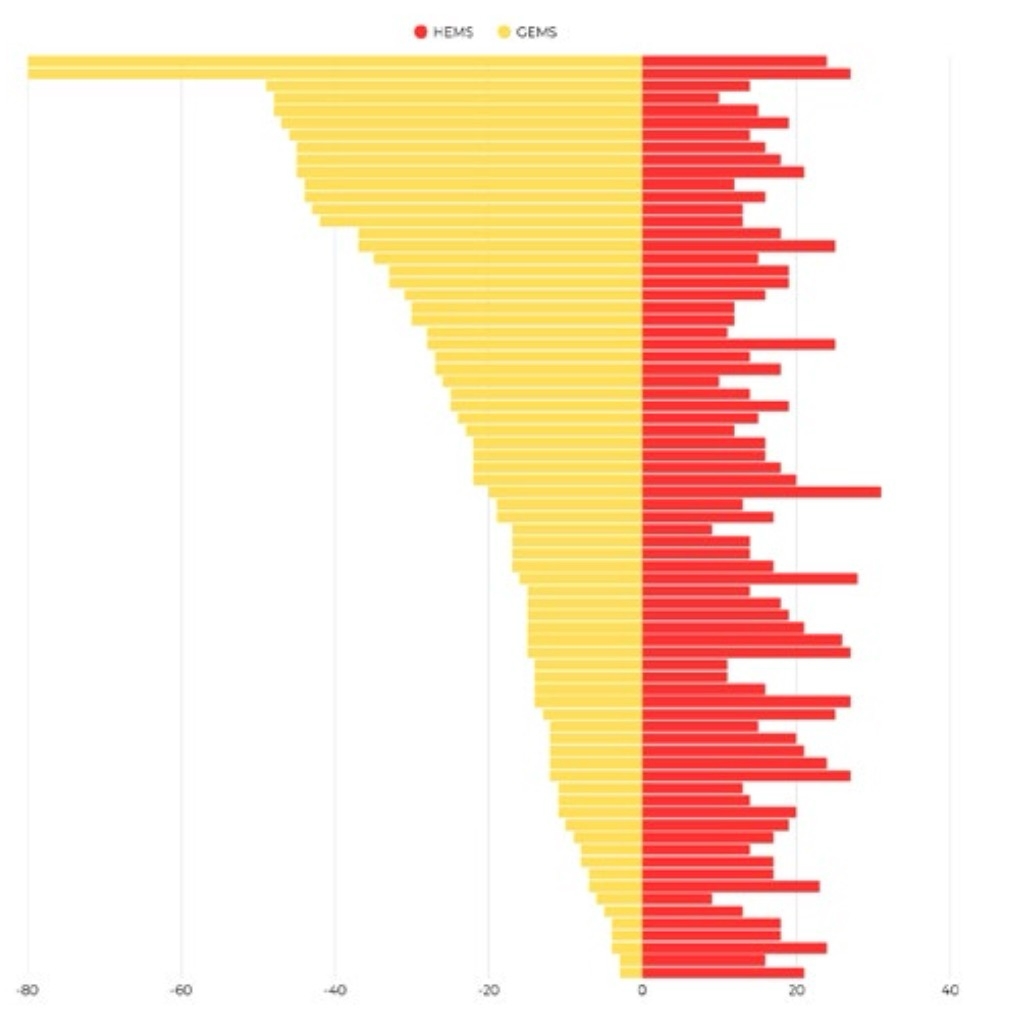
In the analyzed interventions, the median time to transport patients to an appropriate facility that can provide definitive care was 48 minutes for GEMS and 13 minutes for HEMS teams. The patient transport time was shorter with the helicopter team, with a median of 34 minutes for all interventions (Figure 3).
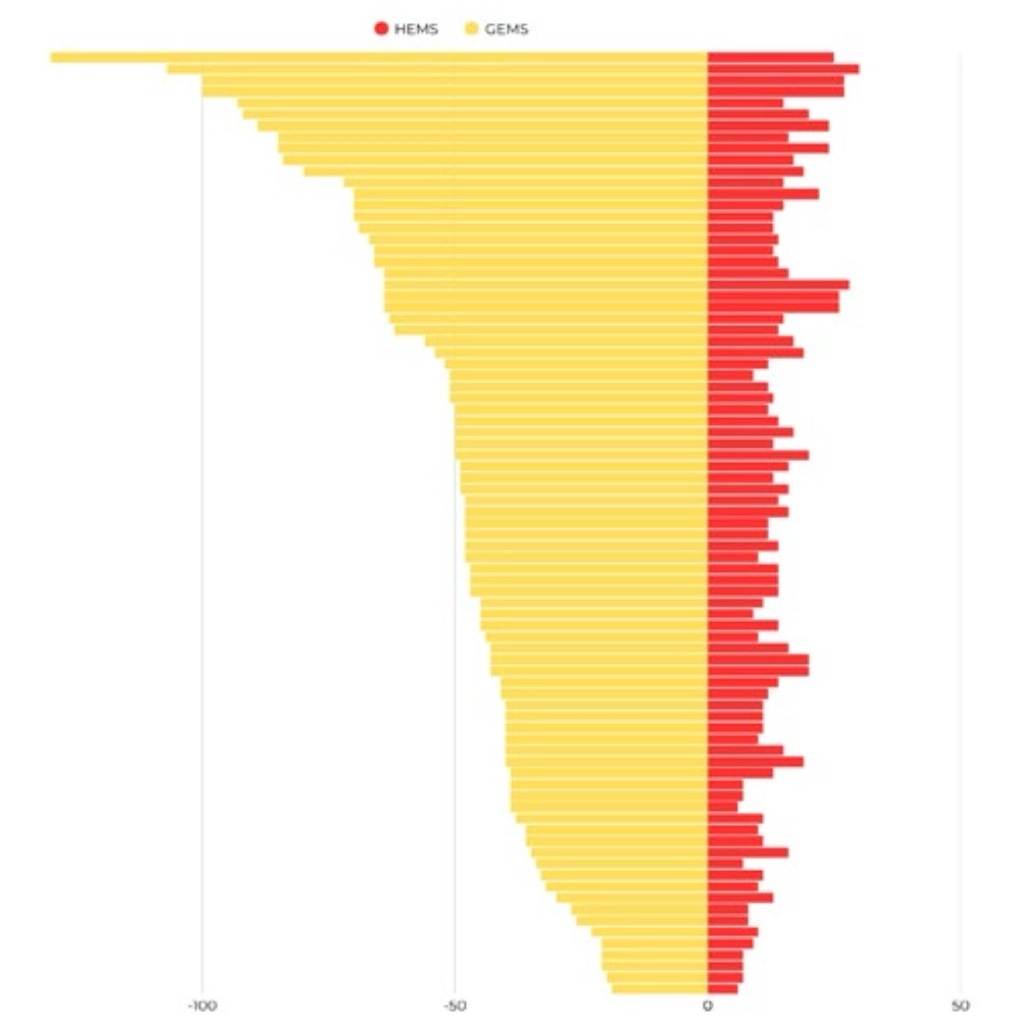
The median duration of the entire intervention was 30 minutes for HEMS versus 70 minutes for GEMS. The median difference in total intervention duration between the HEMS and GEMS teams was 34 minutes (Figure 4).
Based on this, we conclude that the patient care and outcomes of our patients are better due to faster transport and more timely management in an appropriate healthcare facility.
Discussion
Helicopter emergency medical service represents an upgrade to the existing network of ground emergency medical service teams. In most analysed interventions, the time to scene was faster with the helicopter service, but the difference is not statistically significant and depends on geographical specificities of the location, GEMS network distribution, road connectivity and traffic conditions. Statistically significant differences in time to scene of the GEMS and HEMS teams occur in the case of interventions in rural and difficult-to-reach areas.
However, the transport time to an appropriate facility was faster by helicopter in all analyzed interventions, which is expected given the often long distances transport to tertiary centers in Zagreb.
HEMS improves transport times to appropriate facilities, particularly in rural areas, potentially enhancing patient survival despite variable time-to-scene advantages over GEMS.
We do not have data for 30 days mortality for our patients but reviewing the literature, we found evidence that response and transport times and earlier arrival to an appropriate healthcare facility significantly affect patient survival. This finding indicates that patient care for our patients is therefore improved.
The efficiency of the overall treatment of life-threatening patients is additionally conditioned by the organization of the hospital network at the national level. Due to their organizational structure, regional hospitals are not equipped to provide definitive treatment for certain patient conditions, which is why transport to a higher level of care is necessary.
HEMS provides a critical advantage for life-threatening cases in hard-to-reach areas, reducing transport time to specialized care.
Conclusion
The establishment of specialized centers and categorizations, such as trauma centers, cerebrovascular stroke centers, percutaneous coronary intervention centers and burn centers, represents a key step in improving emergency patient care. It is in this context that HEMS fulfills its full clinical and organizational value. The possibility of rapid and direct transport of the patient to a specialized center shortens the total duration of the intervention and reduces the time until the provision of definitive patient care, potentially improving clinical outcomes.
Acknowledgement
The authors would like to express their gratitude to the colleagues who contributed to this study.
Reference
- Guidelines and instructions for medical dispatchers: primary and secondary interventions of HHMS v.4,Croatian Institute for Emergency Medicine,February,2026
- Državni zavod za statistiku. Procjena stanovništva Republike Hrvatske, 2021. STAN-2022-3-1. Zagreb: DZS; 2022.Available from: stan2022-3-1
- Prabhakaran S, Gonzalez NR, Zachrison KS, Adeoye O, Alexandrov AW, Ansari SA et al. Peer Review Committee. 2026 Guideline for the Early Management of Patients With Acute Ischemic Stroke: A Guideline From the American Heart Association/American Stroke Association. Stroke. 2026;. doi: 10.1161/STR.0000000000000513.
- McCoy CE, Chakravarthy B, Lotfipour S. Guidelines for Field Triage of Injured Patients: In conjunction with the Morbidity and Mortality Weekly Report published by the Center for Disease Control and Prevention. West J Emerg Med. 2013;14(1):69-76. doi: 10.5811/westjem.2013.1.15981.
- 5 Queensland Health. Referral pathways: Major trauma (adult). Brisbane: Queensland Health; [n.d.]. Available from: data/assets/pdf_file/0034/873642/referral-pathways-major-trauma-adult. pdf
- Weinlich M, Martus P, Blau MB,Wyen H,Walcher F, Piatek S et al. Competitive advantage gained from the use of helicopter emergency medical services (HEMS) for trauma patients: Evaluation of 1724 patients. Injury. 2019;50(5):1028-1035. doi: 10.1016/j.injury.2018.12.018.
- Meuli L, Zimmermann A, Menges AL, Tissi M, Becker S, Albrecht R et al. Helicopter emergency medical service for time critical interfacility transfers of patients with cardiovascular emergencies. Scand J Trauma Resusc Emerg Med. 2021;29(1):168. doi: 10.1186/s13049-021-00981-4.
- Lichtenberger PM, Peer MF, Lindtner RA, Schneider F, Wallner B, Wagner M. Helicopter vs. ground-based transfer for emergency interhospital transportation: A time and cost-efficiency analysis across varying transfer distances. Injury. 2025;56(7):112359. doi: 10.1016/j.injury.