Introduction
Despite significant advances in diagnosis and treatment, severe infections still represent a major challenge in clinical practice. They are associated with high mortality and the development of organ dysfunction, especially when the source of the infection is not recognized (1). Sepsis is one of the possible consequences of late detectionand treatment of infectious process (2). Recognition and localization of the source of infection are keys to early clinical decision-making in the emergency department. The sources of infection in patients with an unclear clinical presentation are numerous, and most often include the respiratory and urinary systems, intra-abdominal infections, and skin and soft tissue infections (2). Intra-abdominal infections are associated with high morbidity and mortality, especially in the case of delayed control of the source of infection (3). Point-of-care ultrasound (POCUS) has become an indispensable diagnostic tool in modern emergency medicine (4).
Previous research suggests that point-of-care ultrasound can improve the identification of the source of infection compared with initial clinical assessment, with a reported diagnostic accuracy of approximately 80–90 %.”
It is a targeted ultrasound examination performed by a non-radiologist at the patient’s bedside, with the aim of rapid diagnostic orientation, and clinical decision-making (5). Previous research suggests that point-of-care ultrasound can improve the identification of the source of infection compared with initial clinical assessment, with a reported diagnostic accuracy of approximately 80–90 % (3, 6). The aim of our paper is to demonstrate the role of early point-of-care ultrasound in identifying the source of infection in patients with unclear clinical presentation in the emergency department, through the presentation of two clinical cases.
Methods
The paper was a retrospective review of two case reports of patients treated at the Emergency Medicine Center of the University Hospital, in whom POCUS was applied in the early phase of initial workup due to suspected infection of unknown origin. POCUS was performed within the first hour of arrival at the emergency department, before performing advanced imaging tests. The examination was goal-directed and problem-oriented, integrated into the clinical examination. POCUS findings were used for immediate clinical decision-making and preceded the decision on further imaging diagnostics or therapeutic procedures. The ultrasound examination was adapted to the clinical presentation: in the first case, a focused examination of the hepatobiliary system was performed, and in the second, a focused examination of the deep venous system and soft tissues of the lower extremities. The examinations were performed by an emergency medicine specialist with formal education in clinical ultrasound according to the World Interactive Network Focused On Critical UltraSound (WINFOCUS) program.
Case reports
Case report 1
A 75-year-old patient presented to the emergency department due to poor general condition for three days, with fever up to 38.8 °C, chills, and shivering. He had a history of transient epigastric pain with a belt-like spread, but on admission denied abdominal pain. He had no nausea, vomiting, dyspnea, or cough. On admission was conscious, oriented, hemodynamically stable (blood pressure 160/76 mmHg, pulse 75/min, respiratory rate 22/min, oxygen saturation 96%, body temperature 38.5 °C). The abdomen was soft, with audible peristalsis and mild localized tenderness in the right hemiabdomen. Personal history includes aortic valve surgery due to severe aortic stenosis, recovered ischemic cerebrovascular insult, arterial hypertension, and type 2 diabetes. Laboratory findings showed leukocytosis (12.1
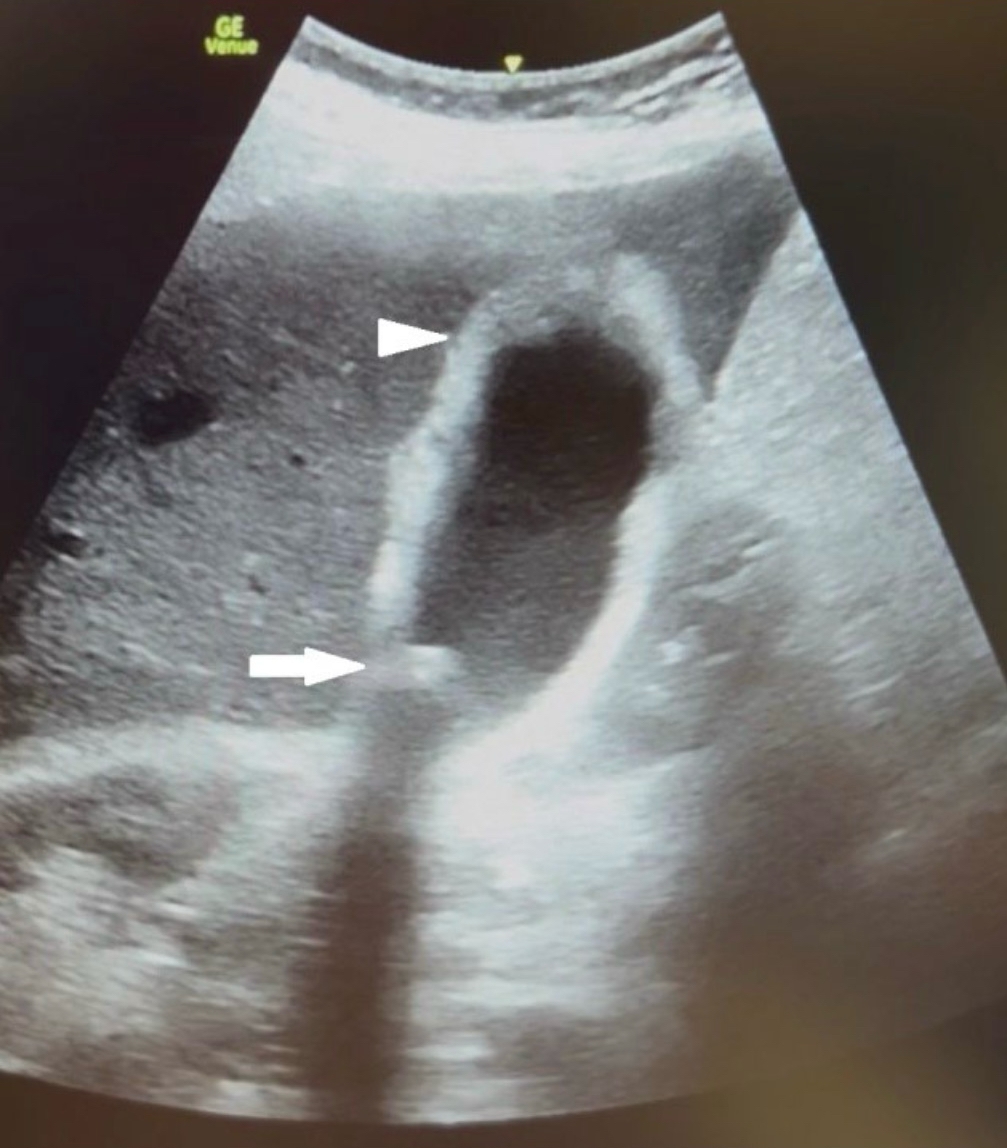
× 10⁹/L), elevated C-reactive protein (CRP) (193.9 mg/L), thrombocytopenia (133 × 10⁹/L), slightly elevated creatinine (114 μmol/L), and elevated total bilirubin. (31.3 μmol/L) and direct bilirubin (11.8 μmol/L). Within 20 minutes of arrival, a POCUS of the abdomen was performed, which showed an enlarged gallbladder (>10 cm) with a thickened and irregular wall (>5 mm), a concretion in the neck of the gallbladder with positive sonographic Murphy’s sign (Figure 1).
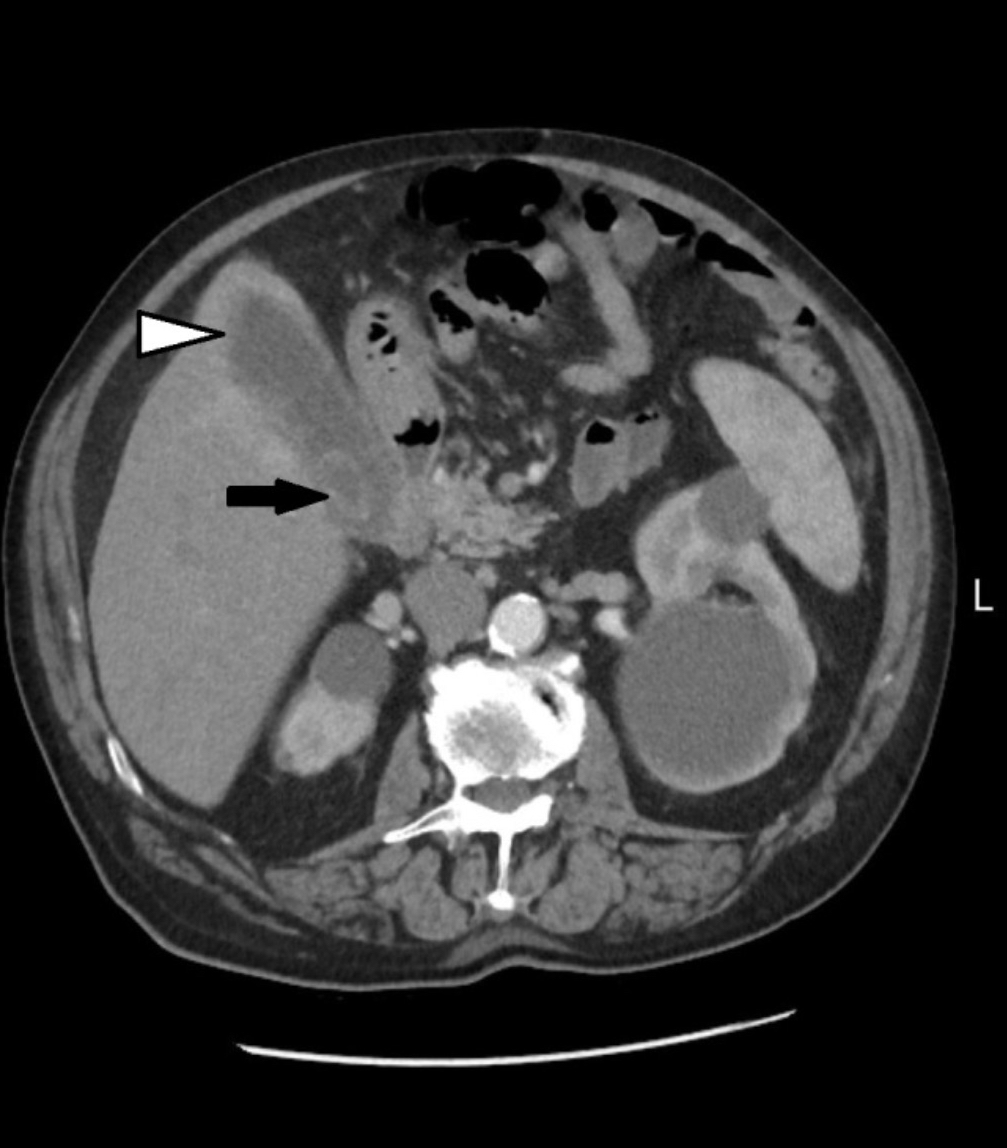
Abdominal multislice computed tomography (MSCT) subsequently confirmed acute gangrenous cholecystitis (Figure 2) and was used for preoperative assessment and surgical planning.
The patient underwent emergency surgery, and the pathohistological findings confirmed the diagnosis of gangrenous cholecystitis with hydrops of the gallbladder. Empiric antibiotic therapy (meropenem) for 7 days was given.
The early application of POCUS enabled rapid identification of the intra-abdominal source of infection, and shortened the time to surgical control of the source of infection despite the atypical clinical presentation.
Case report 2
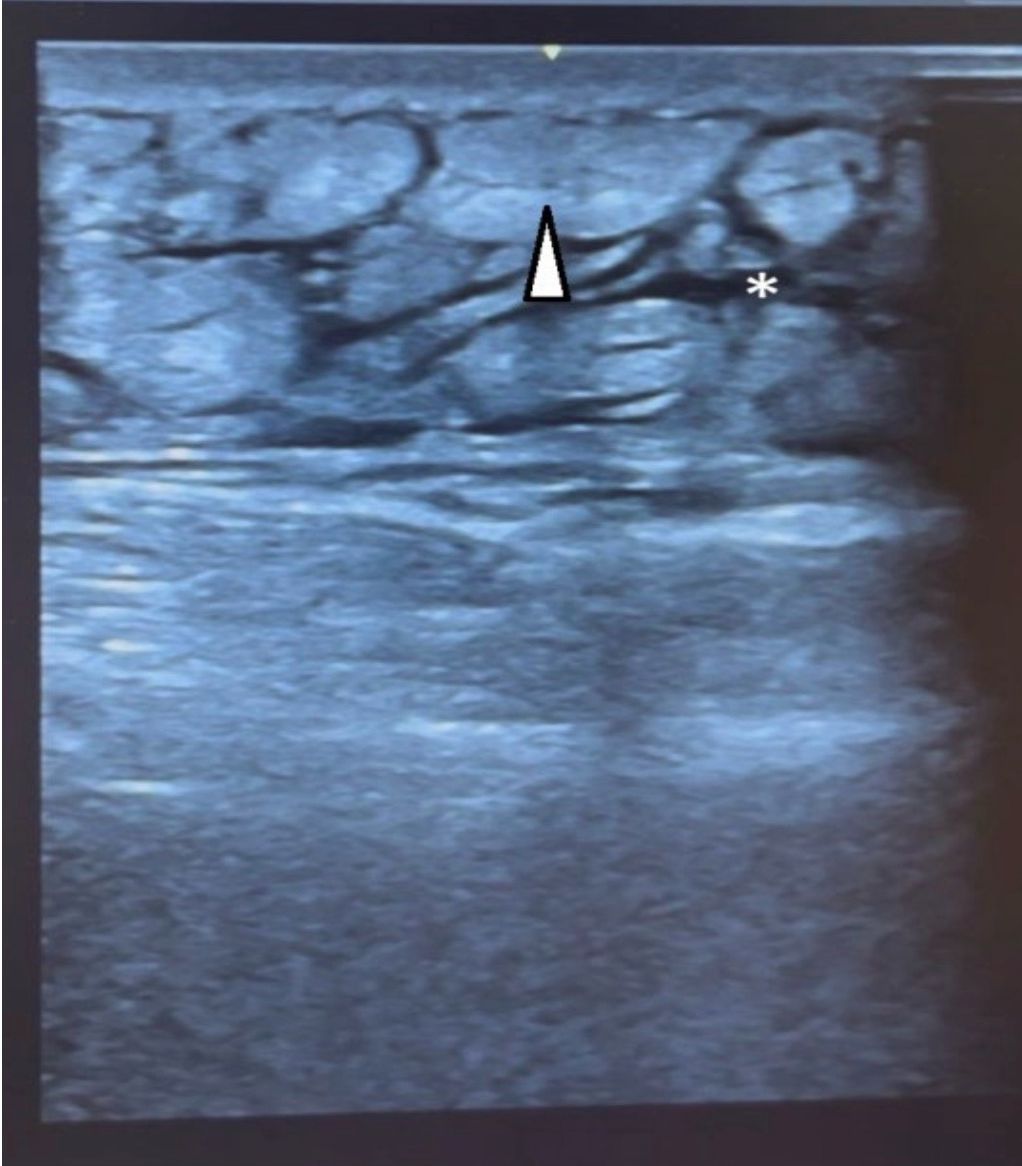
An 80-year-old patient presented to the emergency department with sudden onset of pain and swelling in his left leg that had occurred the day before. Ten days earlier, osteosynthesis of the pertrochanteric femoral fracture had been performed. The postoperative period was uneventful. He now denies trauma. He was afebrile and hemodynamically stable on admission. Clinical examination revealed swelling and tenderness of the left upper leg with warm, taut skin of normal color. Laboratory findings showed leukocytosis (12.7 × 10⁹/L), elevated CRP (124.7 mg/L), and elevated D-dimer (2.63 mg/L). Other findings were within reference values. Deep vein thrombosis was excluded by POCUS examination of the venous system of the lower limb, where the examined veins were properly compressible, without intraluminal echogenic masses. POCUS of the soft tissues of the left upper leg shows thickened and heterogeneous subcutaneous fat tissue with pronounced interstitial edema, a characteristic “cobblestone” appearance, without clearly delimited fluid collections and signs of abscess (Figure 3).
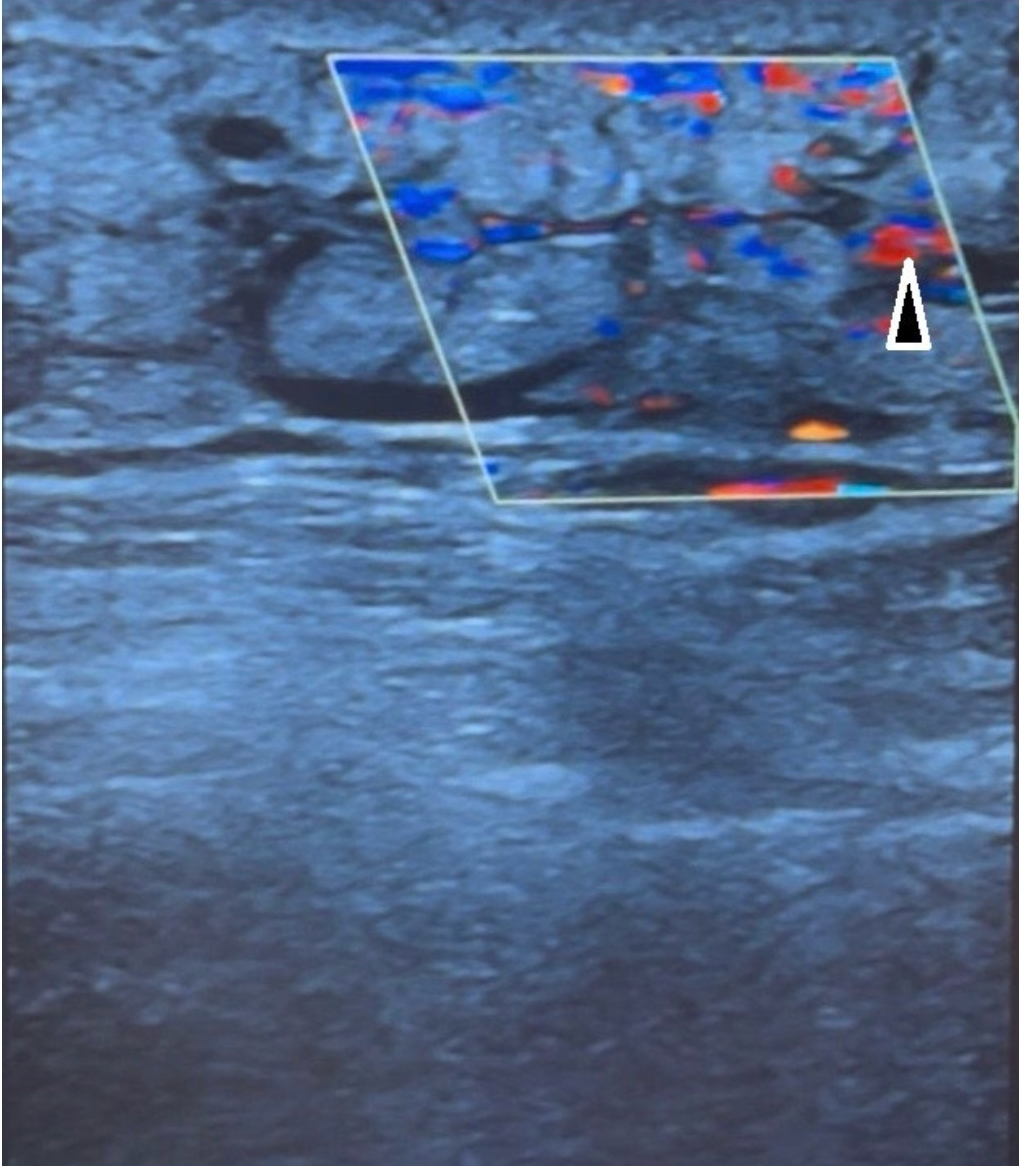
Color Doppler showed increased vascularization of the subcutaneous tissue, which supports an inflammatory etiology.
(Figure 4). The finding was consistent with cellulitis. After the orthopedist’s examination, the patient was admitted to the orthopedics department, where treatment with intravenous antibiotics (ceftriaxone), blood products, and continuation of already prescribed thromboprophylaxis started. During hospitalization, the patient improved with regression of local swelling and a decrease in inflammatory parameters. The use of POCUS enabled the early differentiation of infectious etiology from vascular complications. It also prevented unnecessary additional imaging tests. After 6 days of hospitalization, the patient is discharged home.
Discussion
The presented cases highlight the challenges of early diagnostic work-up of patients with unclear clinical presentation in the emergency department, in whom the initial clinical examination often does not allow reliable localization of the source of infection. In such circumstances, laboratory indicators may indicate the presence of an inflammatory process, but without a clear diagnostic direction. Elevated values of CRP, as a nonspecific marker of inflammation, are often used in this context as a stimulus for further diagnostic work-up (7). In situations requiring rapid clinical decision-making, an accessible diagnostic tool is needed to guide further treatment. POCUS represents an important extension of the clinical examination in the emergency department. It allowed an orientation assessment of possible sources of infection
and the integration of findings into immediate therapeutic decision-making. The difference in Sequential Organ Failure Assessment (SOFA) score between the two patients reflects the different degrees of systemic response to infection at the time of admission. In both cases, POCUS enabled the adaptation of the diagnostic and therapeutic approach to the patient’s clinical presentation, which was in line with the recommendations of the Surviving Sepsis Campaign, which emphasize the importance of timely identification and control of the source of infection (8).
POCUS enabled early differentiation of infectious from vascular etiology and directed further treatment, demonstrating its practical value in patients with unclear clinical presentation in the emergency department.
In the first case presented, POCUS enabled the identification of an intra-abdominal source of infection led to sepsis and prompt surgical control of the infection source. Acute calculous cholecystitis is increasing in incidence in the elderly population, with biliary tract infections, including cholecystitis and cholangitis, being the second most common cause of sepsis and associated with increased morbidity and mortality rates (9). Studies have shown that acute cholecystitis in the geriatric population may present asymptomatically, with patients older than 65 years of age having an increased frequency of atypical clinical presentations (10). In such clinical circumstances, POCUS is a valuable tool because it allows rapid orientation assessment and early suspicion of an intra-abdominal source of infection.According to available data, the sensitivity of POCUS performed by emergency physicians for the diagnosis of acute cholecystitis is 71 % (95 % CI 62–78 %), with a high specificity of 94 % (95 % CI 88–98 %), confirming its reliability as a method for confirmation of the diagnosis (11). MSCT findings in the presented case were consistent with typical radiological features of gangrenous cholecystitis, including gallbladder distension, wall thickening and irregularity, and pericholecystic inflammation (12). In this case, the main contribution of POCUS was not to replace CT, but to reveal the biliary source of infection in a patient with sepsis-like presentation and no dominant abdominal symptoms. By identifying acute cholecystitis early in the emergency department, POCUS redirected further diagnostic and therapeutic management, while MSCT served a complementary role in preoperative assessment and surgical planning.
In the second presented case, POCUS played major role in the differential diagnosis of patients with elevated inflammatory parameters and localized symptoms on the lower extremity. The clinical presentation with sudden swelling and pain in the leg, with elevated D-dimer values, justified the suspicion of deep vein thrombosis. However, point-of-care ultrasound ruled out thrombosis already in the early stages of treatmentwhile ultrasound examination of soft tissues showed diffuse edema with pronounced hypervascularization of the subcutaneous tissue, in accordance with the diagnosis of cellulitis. The use of POCUS enabled early differentiation of infectious from vascular etiology and directed further treatment. In the differential diagnosis of soft tissue infections, POCUS shows a high sensitivity of 95 % (95% CI 89–97 %) and specificity of 85 % (95% CI 79–90 %) for the detection of abscesses versus cellulitis, enabling quick and safe clinical decision-making without the need for additional tests (13).Serum lactate was not measured in any case because the patients had no clinical or hemodynamic signs of septic shock, and the diagnosis of sepsis in the first case was based on proven infection and present organ dysfunction assessed by the SOFA score, in accordance with the recommendations of the Surviving Sepsis Campaign guidelines (8).The presented cases confirm the practical value of problem-oriented POCUS applicationin the treatment of patients with an unclear clinical presentation in the emergency department. In both cases, the ultrasound findings were integrated into the overall clinical assessment and played a role in guiding further diagnostic and therapeutic treatment, emphasizing its function as a tool for clinical decision-making, and not as a substitute for standard imaging methods.
Conclusion
Point-of-care ultrasound is a valuable addition to the clinical examination in the management of patients with unclear clinical presentations in emergency medicine. In the presented cases, the problem-oriented application of POCUS enabled the identification of the source of infection, guided further diagnostic and therapeutic management in patients at different stages of the infectious process. These examples, from everyday clinical practice, indicate the importance of targeted and systematic educationemergency physicians withPOCUS usein the clinical decision-making process. Despite the limitations associated with the retrospective design and small number of studies, this study indicates the need for future prospective studies to assess the impact of POCUS on decision-making and time to control the source of infection.
Ethics statement
This case report was carried out in full compliance with ethical research guidelines. Informed consent to publish was obtained priorto publication, and measures were taken to safeguard the privacy and maintain confidentiality of the data presented.
Disclosure
The authors declare that no funds, grants, or other support were received during the preparation of this manuscript. The authors declare they have no financial interests.
Reference
- Sweeney DA, Wiley BM. Integrated Multiorgan Bedside Ultrasound for the Diagnosis and Management of Sepsis and Septic Shock. Semin Respir Crit Care Med. 2021;42(5):641-649. doi: 10.1055/s-0041-1733896.
- Long B, Gottlieb M. Emergency medicine updates: Evaluation and diagnosis of sepsis and septic shock. Am J Emerg Med. 2025;90:169-178. doi: 10.1016/j. ajem.2025.01.055.
- Hecker A, Reichert M, Reuß CJ, Schmoch T, Riedel JG, Schneck E et al. Intra-abdominal sepsis: new definitions and current clinical standards. Langenbecks Arch Surg. 2019;404(3):257-271. doi: 10.1007/s00423-019-01752-7.
- Osterwalder J, Polyzogopoulou E, Hoffmann B. Point-of-Care Ultrasound-History, Current and Evolving Clinical Concepts in Emergency Medicine. Medicina (Kaunas). 2023;59(12):2179. doi: 10.3390/medicina59122179.
- Radonjić T, Popović M, Zdravković M, Jovanović I, Popadić V, Crnokrak B et al. Point-of-Care Abdominal Ultrasonography (POCUS) on the Way to the Right and Rapid Diagnosis. Diagnostics (Basel). 2022;12(9):2052. doi: 10.3390/ diagnostics12092052.
- Polyzogopoulou E, Velliou M, Verras C, Ventoulis I, Parissis J, Osterwalder J et al. Point-of-Care Ultrasound: A Multimodal Tool for the Management of Sepsis in the Emergency Department. Medicina (Kaunas). 2023;59(6):1180. doi: 10.3390/ medicina59061180.
- Póvoa P. C-reactive protein: a valuable marker of sepsis. Intensive Care Med. 2002;28(3):235-43. doi: 10.1007/s00134-002-1209-6.
- Evans L, Rhodes A, Alhazzani W, Antonelli M, Coopersmith CM, French C et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock 2021. Intensive Care Med. 2021;47(11):1181-1247. doi: 10.1007/ s00134-021-06506-y.
- Sermonesi G, Rampini A, Convertini G, Bova R, Zanini N, Bertelli R et al. Biliary Sepsis Due to Recurrent Acute Calculus Cholecystitis (ACC) in a High Surgical-Risk Elderly Patient: An Unexpected Complication. Pathogens. 2022;11(12):1423. doi: 10.3390/pathogens11121423.
- Aleman Espino E, Kazaleh M, Zaglul J, Frontela O.Acute Cholecystitis Presenting With Atypical Radiologic or Laboratory Findings: A Case Report. Cureus. 2023;15(6):e41217. doi: 10.7759/cureus.41217.
- Wilson SJ, Thavanathan R, Cheng W, Stuart J, Kim DJ, Glen P et al. Test Characteristics of Emergency Medicine-Performed Point-of-Care Ultrasound for the Diagnosis of Acute Cholecystitis: A Systematic Review and Meta-analysis.Ann Emerg Med. 2024 Mar;83(3):235-246. doi: 10.1016/j.annemergmed.2023.09.005.
- Bennett GL, Rusinek H, Lisi V, Israel GM, Krinsky GA, Slywotzky CM et al. CT findings in acute gangrenous cholecystitis. AJR Am J Roentgenol. 2002;178(2):275-81. doi: 10.2214/ajr.178.2.1780275.
- Gottlieb M, Avila J, Chottiner M, Peksa GD. Point-of-Care Ultrasonography for the Diagnosis of Skin and Soft Tissue Abscesses: A Systematic Review and Meta-analysis. Ann Emerg Med. 2020;76(1):67-77. doi: 10.1016/j. annemergmed.2020.01.004.