Introduction
Cold-induced collapse and successful resuscitation have long been reported, leading to hypothermia’s recognition as a unique scenario in advanced life support guidelines by the late 20th century (1). Key statements established that even seemingly lifeless hypothermic patients may survive with persistent resuscitation and controlled rewarming—principles now standard in modern protocols (1,2). Research in the 1980s and 1990s further detailed the physiological progression of hypothermia and shaped current rewarming and extracorporeal referral recommendations (1,3). Accidental hypothermia is defined as an unintentional drop in core temperature below 35°C. It is categorised into three stages (Table 1), each indicating increasing physiological compromise. These categories are used in clinical protocols and guidelines to guide rewarming and adapt resuscitation approaches, corresponding to specific physiological changes in emergency care (1,2).
Patients with severe accidental hypothermia, even those presenting without detectable vital signs, may achieve full recovery if subjected to sustained resuscitation and controlled rewarming
Accidental hypothermia affects all climates yearround and impacts urban and rural populations. Atrisk groups include the homeless, older adults, those with substance use disorders, outdoor enthusiasts, trauma victims, and individuals submerged in cold water. Its global epidemiology is shaped by environmental and socioeconomic factors (1,2). Hypothermia commonly presents in emergency settings and, especially in trauma, is part of the “lethal triad” (with coagulopathy and acidosis), predicting higher mortality and requiring prompt recognition and prevention of further heat loss (1,10). Severe hypothermia suppresses cardiac and cerebral function, raising the risk of
dangerous arrhythmias and arrest, so emergency protocols must include early internal or extracorporeal rewarming for unstable patients (1,2). Advances in extracorporeal methods have notably improved outcomes and are now central to hypothermia management (2).
Objectives of this review seek to outline current consensus definitions and temperaturebased staging systems that inform clinical decisionmaking, provide an integrated overview of the pathophysiologic changes affecting multiple organ systems, with particular attention to their relevance in emergency care, present severitybased diagnostic and management pathways, including criteria for initiating ECLS or cardiopulmonary bypass, summarize characteristic laboratory abnormalities and ECG findings that influence prognosis and therapeutic choices, discuss considerations for highrisk or special populations, including paediatric, geriatric, and trauma patients and finally evaluate existing evidencebased guidelines and highlight key gaps requiring further research. A narrative review was conducted, sourcing data from peer-reviewed articles, surveys, observational studies, and guidelines via PubMed, covering definitions, physiology, epidemiology, and treatment.
Pathophysiology
Thermoregulation and Compensatory Mechanisms
Core temperature is maintained by balancing heat production (metabolism, shivering) with heat loss, regulated by hypothalamic control and autonomic responses such as vasoconstriction and sympathetic activation. When heat loss exceeds production, core temperature drops. Early compensatory mechanisms include shivering, vasoconstriction, increased metabolic rate, and sympathetic drive. With further cooling, these responses fail—shivering stops, metabolism slows, mental status declines, and cardiovascular depression develops.
Mechanisms of Heat Loss
Heat is lost through four pathways (table 3.)
Rapid cooling occurs with icy-water immersion (<5°C), wet clothing, and wind exposure. Exact realworld contributions of each mechanism remain poorly quantified.
Cardiovascular Changes by Temperature Stage
With a drop in body temperature, the cardiovascular system undergoes changes ranging from barely noticeable to profound, with fatal consequences if hypothermia is not controlled.
These changes form the basis for modified ACLS recommendations in hypothermia.
Respiratory Effects
Cold exposure initially increases respiratory rate, followed by slow, shallow breathing as cooling progresses. Severe hypothermia causes hypoventilation, hypoxemia, and hypercapnia. Reduced metabolic rate lowers oxygen demand, but hypothermia combined with hypoxia (e.g., drowning) worsens outcomes.
Neurological Manifestations
Cooling progressively reduces cerebral metabolism and blood flow:
• Mild: Confusion, slowed cognition
• Moderate: Stupor, diminished reflexes
• Severe: Coma with minimal signs of life
Profound hypothermia may mimic death, supporting the principle of continuing resuscitation until rewarmed unless clear signs of irreversible death exist.
Metabolic Alterations
Hypothermia causes:
• Reduced metabolic rate
• Impaired insulin release and altered glucose handling
• Metabolic acidosis
• Slowed drug metabolism
• Electrolyte shifts, especially potassium abnormalities
Electrolyte Abnormalities
• Hyperkalaemia: Common during rewarming; very high levels predict poor prognosis.
• Hypokalaemia: May result from cold diuresis.
• Additional disturbances in sodium, calcium, and magnesium may occur. Hyperkalemia is sometimes used to guide decisions about aggressive rewarming or ECLS candidacy.
Renal and Endocrine Effects
• Reduced renal blood flow and vasoconstriction impair kidney function.
• Cold diuresis from central volume shifts and reduced ADH contributes to hypovolemia and electrolyte loss.
• Early catecholamine and cortisol release may diminish in severe hypothermia.
• Preexisting thyroid or adrenal insufficiency may worsen.
Coagulation Abnormalities
Hypothermia impairs haemostasis through platelet dysfunction, slowed enzymatic activity, prolonged clotting times, and increased bleeding risk. These issues are critical in trauma and during ECMO, where anticoagulation is required.
Afterdrop Phenomenon
Afterdrop is a continued fall in core temperature during early rewarming due to cold peripheral blood returning centrally. It is minimized by controlled rewarming and avoiding rapid peripheral vasodilation. Close monitoring during transport and early rewarming is essential.
Implications for Emergency Management
Physiologic stage guides rewarming strategy:
• Mild: Passive or active external warming
• Moderate: Active external ± internal warming
• Severe or unstable: Active internal rewarming and consideration of extracorporeal life support/ cardiopulmonary bypass (ECLS/CPB)
Extracorporeal techniques provide circulatory support and controlled rewarming, improving survival in severe hypothermic arrest. Impaired drug metabolism at low temperatures requires ACLS medication adjustments when core temperature is <30°C.
In severe or unstable hypothermia, timely internal rewarming potentially with extracorporeal support is critical to restore circulation and improve survival.
Clinical presentation and diagnosis
Clinical Signs by Severity
Clinical changes vary according to the level of hypothermia, ranging from shivering and vasoconstriction to the development of coma and pronounced bradycardia.
Electrocardiographic Findings
ECG monitoring is essential. Key features:
• Osborn ( J) waves: Classic in moderate–severe hypothermia; correlate with lower temperature and higher arrhythmia risk.
• Other changes: Bradyarrhythmias, prolonged PR/QRS/ QT, atrial fibrillation, ventricular arrhythmias (<28°C).
• Refractory myocardium: Limited response to drugs and defibrillation until rewarmed.
Core Temperature Measurement
Preferred methods: Esophageal (during resuscitation), rectal, bladder, lowtemperature tympanic probes. Avoid: Oral, axillary, standard tympanic, skin readings. Note: Do not delay transport or rewarming; obtain core temperature early in the emergency department.
Laboratory Abnormalities
Laboratory abnormalities in hypothermia are shown in the table below.
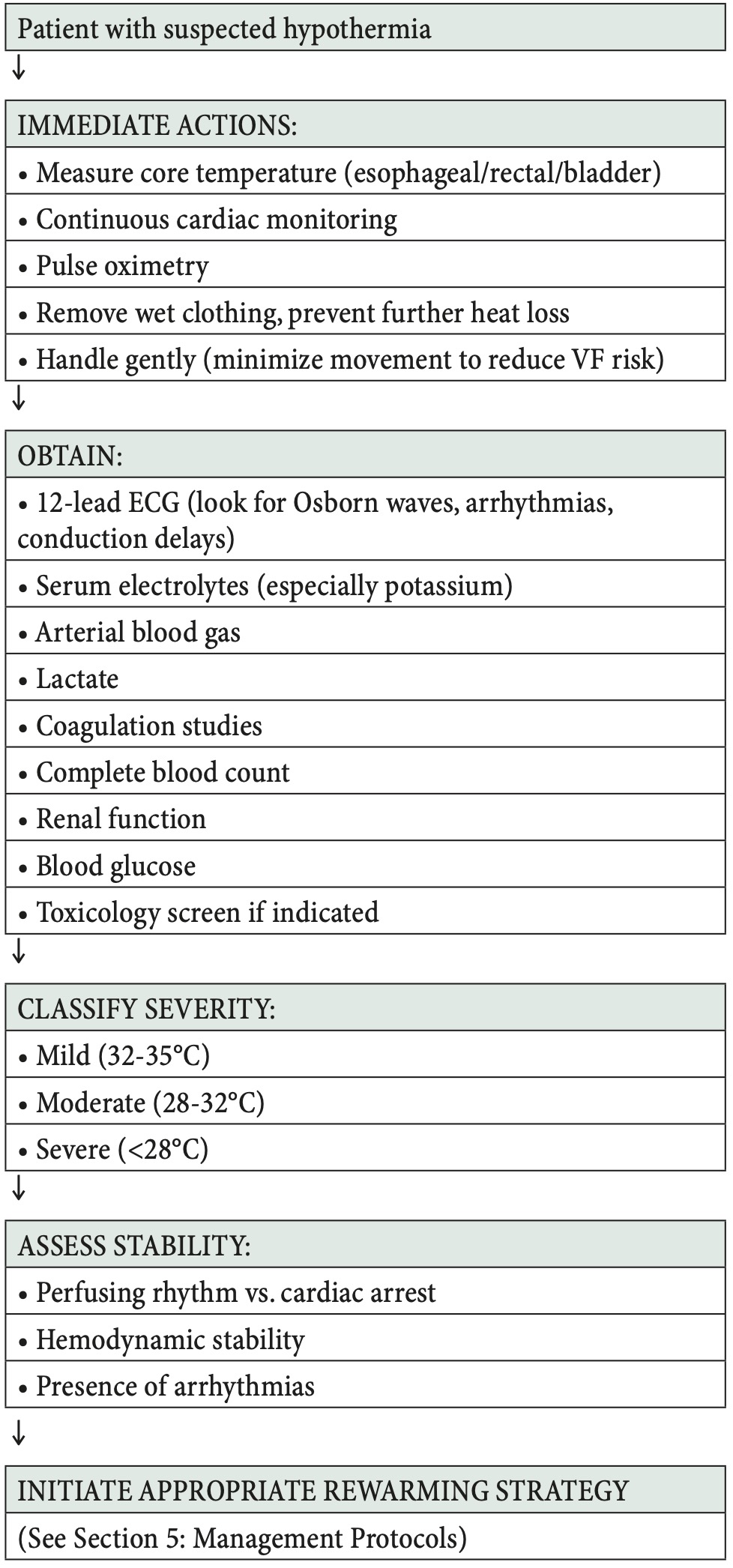
Prompt action following the hypothermia diagnostic algorithm on patient arrival in the emergency department is crucial to prevent complicatons. (see Figure 1. below)
Differential diagnosis
Accidental hypothermia may result from direct environmental exposure—such as prolonged cold exposure, homelessness, outdoor activity, or coldwater immersion (1,12)—but can also reflect underlying medical conditions. Endocrine disorders, sepsis, neurologic injury, toxicologic impairment, metabolic derangements, and dermatologic disease may all contribute to or mimic hypothermia (1,4,16). Iatrogenic factors, including perioperative cooling, unwarmed transfusions, and therapeutic hypothermia protocols, are additional considerations (1,17). Evaluation must account for both primary and secondary causes, and in infants, hypothermia should prompt assessment for serious bacterial infection (18).
Risk factors and etiology
Accidental hypothermia is mainly caused by environmental exposure—prolonged cold, poor shelter, wilderness or work exposure, and cold-water immersion, which rapidly lowers body temperature (1,12). Submersion combines hypothermia with hypoxia; rapid cooling may sometimes protect the brain during arrest (1,6). Annually, about 1,300 deaths occur in the U.S., and 2–5 per 100,000 in Europe, though true rates are likely underestimated due to coding
Emergency Department Initial Assessment
The primary survey follows standard airway, breathing, and circulation (ABC) protocols with hypothermia-specific modifications (1). Airway patency assessment and intubation for unconsciousness or inadequate ventilation, supplemental oxygen provision (preferably heated and humidified), and circulation assessment requiring prolonged pulse checks (30-45 seconds) are essential (1). Vascular access establishment and cardiac monitoring initiation complete the primary survey (1). Immediate interventions include continuous cardiac monitoring for arrhythmia detection (particularly ventricular fibrillation/ventricular tachycardia), core temperature measurement via oesophageal, rectal, or bladder probe, 12-lead electrocardiography to document rhythm and identify Osborn waves, prevention of further heat loss through removal of wet clothing and application of warm blankets, gentle handling to minimize movement, and establishment of intravenous access (preferably central for warmed fluid administration) (1,4).
Essential laboratory studies comprise serum electrolytes (with particular attention to potassium), arterial blood gas analysis, lactate, complete blood count, coagulation studies (prothrombin time/international normalized ratio, activated partial thromboplastin time), renal function assessment (creatinine, blood urea nitrogen), creatine kinase if rhabdomyolysis is suspected, blood glucose, and toxicology screening when indicated (1,4). Prognostic markers include serum potassium, with markedly elevated nonhemolyzed values (>10-12 mmol/L) associated with poor outcomes and used as a triage consideration in some protocols (1,2). Elevated lactate correlates with severity and mortality, while severe acidosis predicts worse outcomes (1,2).
Rewarming Strategies Overview
Rewarming strategies are selected based on hypothermia severity and hemodynamic stability. Passive external rewarming, appropriate for mild hypothermia (32-35°C) with stable vital signs, achieves rewarming rates of 0.5-2°C per hour through insulation, warm environment, and wet clothing removal (1). Active external rewarming, indicated for moderate hypothermia or inadequate passive rewarming response, utilizes forced-air warming systems, heating blankets, radiant heaters, and warm packs applied to the trunk, achieving rates of 1-2.5°C per hour (4). Active internal rewarming (non-ECMO), employed for moderate to severe hypothermia without ECLS indications, incorporates warmed intravenous fluids (42-44°C), heated humidified oxygen (42-46°C), gastric/bladder lavage, peritoneal lavage, pleural lavage, and intravascular warming catheters, with rewarming rates of 1-3°C per hour (1,4,20). Extracorporeal rewarming (ECLS/ECMO), recommended for cardiac arrest, severe hypothermia (<28°C) with unstable circulation, or refractory ventricular arrhythmias, achieves the most rapid rewarming (3-10°C per hour) and demonstrates marked survival improvements in case series (2,14).
Passive Rewarming
Passive rewarming serves as the initial step for all hypothermic patients and may suffice as sole therapy for mild cases (32-35°C) with stable hemodynamics (1,4). Techniques include removal of all wet clothing, insulation with dry blankets or sleeping bags, ambient room temperature elevation (25-28°C), head covering to prevent scalp heat loss, and vapor barrier application to reduce evaporative losses (1). Monitoring includes serial core temperature measurements every 15-30 minutes, continuous cardiac monitoring, vital signs assessment, and mental status evaluation (4). Limitations include slow rewarming rates (0.5-2°C per hour) and insufficiency for severe hypothermia (1).
Active External Rewarming
Active external rewarming is indicated for moderate hypothermia (28-32°C), mild hypothermia inadequately responding to passive methods, or as an adjunct to active internal rewarming in severe cases (4). Forced-air warming systems (e.g., Bair Hugger, Warm Touch), the most common method in modern emergency departments, apply warming blankets preferentially to the trunk at temperatures of 40-43°C (4). Conductive heating blankets utilizing circulating warm water, radiant overhead warming lights, and warm packs applied to trunk areas (axillae, groin, neck) provide additional options (1,4). Precautions include afterdrop monitoring, wherein peripheral vasodilation returns cold blood to the core causing transient temperature decrease, thermal injury surveillance for burns particularly in patients with altered sensation, and rewarming shock management with intravenous fluid preparation for vasodilation-induced hypotension (1,4).
Active Core Rewarming: Warmed Intravenous Fluids
Warmed intravenous fluid administration is indicated for moderate to severe hypothermia, all patients requiring
intravenous resuscitation, and as an adjunct to other
rewarming methods (1). Isotonic crystalloids (normal saline or lactated Ringer’s solution) warmed to 42-44°C are delivered via fluid warmers, with central venous administration preferred in severe cases at rates typically of 150-200 mL per hour, adjusted based on hemodynamics and volume status (1). Precautions include volume overload monitoring for pulmonary oedema, electrolyte shift surveillance (particularly potassium), and avoidance of peripheral intravenous access in severe cases due to poor extremity perfusion (1,4).
Active Core Rewarming: Heated Humidified Oxygen
Heated humidified oxygen (42-46°C) is indicated for all intubated hypothermic patients and spontaneously
breathing patients with severe hypothermia when
equipment is available (1). Delivery occurs via ventilator circuit or high-flow nasal cannula systems with essential humidification to prevent airway desiccation (1). Benefits include airway and core warming, respiratory heat loss prevention, oxygenation support, relative non-invasiveness, and compatibility with all other rewarming methods (1).
Active Core Rewarming: Body Cavity Lavage
Gastric and bladder lavage, involving warmed saline (40-42°C) instillation via nasogastric tube or urinary catheter, provides limited contribution to core rewarming due to restricted surface area and serves only an adjunctive role
(1). Peritoneal lavage (peritoneal dialysis) is indicated for severe hypothermia when ECLS is unavailable (1,4). Technique involves peritoneal dialysis catheter insertion, instillation of warmed (approximately 43°C) potassium-free dialysis fluid in 2-liter volumes with 20-30 minute dwell times, followed by drainage and repetition (1,4). The large surface area for heat exchange and feasibility in most hospitals constitute advantages, while invasiveness, perforation risk, infection risk, and slower rewarming compared to ECMO represent disadvantages (1). Pleural/ thoracic lavage is indicated for severe hypothermia, especially with cardiac arrest, when ECLS is unavailable (1,21). Bilateral chest tube placement (typically 36-40 French), warmed normal saline (40-42°C) instillation into one hemithorax with drainage from the contralateral chest tube in volumes of 300-500 mL per exchange characterize the technique (1,21). Greater effectiveness than peritoneal lavage due to cardiac and great vessel proximity represents an advantage, while high invasiveness, chest tube placement requirements, and risks of pneumothorax, haemothorax, and infection constitute disadvantages (1,21). Case reports and small series demonstrate feasibility and success (21).
Active Core Rewarming: Intravascular Warming Devices
Endovascular warming catheters placed in central veins (femoral, internal jugular) circulate warm saline through balloon or coil structures to achieve direct blood warming
(20). Indications include severe hypothermia and situations requiring an intermediate option between external methods and ECMO when ECMO is not immediately available (20). Advantages encompass less invasiveness than ECMO, controlled rewarming rates (1-3°C per hour), emergency department or intensive care unit placement capability, and elimination of perfusionist or cardiac surgery team requirements (20). Disadvantages include central venous access and expertise requirements, slower rewarming than ECMO, absence of hemodynamic support, and limited center availability (20). A growing body of literature supports efficacy, though comparative outcome data versus ECMO remain limited (20).
Extracorporeal Life Support and Cardiopulmonary Bypass
Strong indications for ECLS include hypothermic cardiac arrest (ventricular fibrillation, ventricular tachycardia, pulseless electrical activity, or asystole), severe hypothermia (<28°C) with hemodynamic instability, refractory ventricular arrhythmias, or hypotension unresponsive to fluids and vasopressors, and moderate hypothermia (28-32°C) with cardiac arrest or severe cardiovascular instability (1,2,14). Relative contraindications include very high nonhemolyzed serum potassium (>10-12 mmol/L in some protocols), lethal injuries incompatible with survival, known terminal illness, prolonged warm cardiac arrest prior to cooling, and evidence of tissue necrosis suggesting prolonged exposure with irreversible damage, though clinical judgment is required as some patients with elevated potassium have survived with ECLS (1,2).
Resuscitation Modifications in Hypothermia
For core temperatures <30°C, repeated resuscitation drug boluses are generally withheld due to altered metabolism and risk of toxicity upon rewarming (1). At 30–35°C, if drugs are used, dosing intervals should be doubled (applies to epinephrine, amiodarone, lidocaine, atropine)
(1). Defibrillation: Up to three shocks for ventricular fibrillation/tachycardia; further attempts deferred until core temperature >30°C (some protocols use 32°C) (1). Continue CPR during rewarming; prolonged resuscitation is justified due to neuroprotective effects (“no one is dead until they are warm and dead”) (1,2). Pulse checks may require 30–45 seconds due to bradycardia; consider mechanical CPR for extended resuscitation or transport (1,2). Termination criteria are not well-defined: consider exposure duration, serum potassium (>10–12 mmol/L), lethal injuries, frozen body cavities, and clear signs of death. Resuscitation should continue until rewarming to at least 32–35°C unless irreversible death is evident (1,2). Criteria for resuscitation termination are not well-defined but should consider exposure duration, serum potassium (>10-12 mmol/L), evidence of lethal injuries, frozen body cavities, and obvious signs of death (rigor mortis, dependent lividity), with the general principle of continuing resuscitation until rewarming to at least 32-35°C unless clear evidence of irreversible death exists (1,2).
Severe hypothermia with hemodynamic instability or cardiac arrest requires rapid active internal rewarming, preferably with extracorporeal life support (ECLS/ ECMO), to restore circulation and improve survival.
Airway Management
Intubation is indicated for unconsciousness (Glasgow Coma Scale ≤8), inadequate ventilation, inability to protect airway, cardiac arrest, and severe hypoxemia (1). Technique considerations include gentle laryngoscopy to avoid excessive stimulation potentially precipitating ventricular fibrillation, preoxygenation with warmed humidified oxygen when available, rapid sequence intubation modifications considering hemodynamic effects of induction agents, and post-intubation provision of heated humidified oxygen via ventilator circuit (1).
Fluid Resuscitation
All intravenous fluids should be warmed (42-44°C) using fluid warmers or rapid infusion systems, with central venous access preferred in severe hypothermia (1). Initial resuscitation is guided by hemodynamics, with anticipation of shifts during rewarming as vasodilation causes relative hypovolemia (1). Careful monitoring is required to avoid both under-resuscitation and pulmonary edema, while excessive crystalloid administration may worsen hypothermia-induced coagulopathy (1,10). Blood products, indicated for trauma, ongoing bleeding, or severe anemia, must be warmed, with anticipation of worsened coagulation necessitating early use of plasma, platelets, and tranexamic acid in trauma (10).
Special populations
Pediatric Hypothermia
Neonates and infants (≤90 days) demonstrate unique vulnerabilities including high surface area-to-volume ratio causing rapid heat loss, immature thermoregulation, limited shivering ability, dependence on brown fat thermogenesis, and thin subcutaneous fat layers (18). Hypothermia in young infants may indicate serious bacterial or viral infection, with emergency department practice showing high variability and substantially greater rates of invasive testing in infants ≤30 days, including blood cultures, urine cultures, lumbar puncture for cerebrospinal fluid analysis, and empirical antibiotics (18). Older children demonstrate better thermoregulation than infants but remain vulnerable, with behavioral factors (inadequate clothing, water play) and submersion incidents representing common causes
(1). Management follows adult principles scaled to size with lower threshold for ECLS consideration in paediatric centers and essential family-centered care (1).
Neonates and young infants are highly vulnerable to hypothermia due to immature thermoregulation, high surface area-to-volume ratio, and limited shivering, and hypothermia in this age group may indicate serious infection.
Trauma-Associated Hypothermia
Hypothermia is part of the trauma “lethal triad” (hypothermia → coagulopathy → acidosis), with each factor worsening the others (10). Causes include prolonged scene time, clothing removal, haemorrhagic shock, cold environment, room-temperature IV fluids, open wounds, and cold operating rooms (10). Each 1°C drop below 35°C increases mortality, transfusion needs, coagulation times, acidosis, platelet dysfunction, and length of hospital/ICU stay (1,10). Prevention: minimize scene time, remove wet clothing, use blankets/insulation, warm ambulance, and give warmed IV fluids when possible (10). Emergency department: warm resuscitation bay, remove clothing only as needed, cover exposed areas, use forced-air warming, give warmed fluids/blood, provide heated humidified oxygen, and limit unnecessary exposure (10). Operating room: increase ambient temperature, use forced-air warming, warmed irrigation fluids, warmed IV fluids/blood, and minimize surgical time (damage control principles) (10).
Submersion and Cold-Water Immersion
Water conducts heat 25 times faster than air, with immersion in icy water (<5°C) causing profound hypothermia within minutes and core temperature dropping 1-2°C within the first few minutes (1,6). The cold-water immersion sequence progresses through cold shock response (0-3 minutes) with gasping, hyperventilation, and tachycardia; cold incapacitation (3-30 minutes) with loss of muscle function and inability to swim; hypothermia (>30 minutes) with progressive cooling and altered consciousness; and circum-rescue collapse with cardiac arrest during or immediately after rescue (1). Rapid cooling may reduce cerebral metabolic rate before severe hypoxia, potentially explaining rare cases of good neurological recovery after prolonged submersion, with maximal protection in very cold water (<5°C) with rapid submersion (1,22).
Outcomes and prognosis
Cardiac Arrest Outcomes
Pre-ECLS era survival from hypothermic cardiac arrest typically remained below 50%, limited by conventional rewarming methods’ inability to provide circulatory support (2). Contemporary ECLS era outcomes demonstrate survival approaching 100% in highly selected patients (young, previously healthy, witnessed arrest, rapid CPR initiation, rapid ECLS access, no prolonged warm cardiac arrest) (2,22), while real-world multicentre data reveal more variable outcomes with survival rates of 30-70% depending on patient selection and system factors, better outcomes in specialized centres with established protocols, and selection bias in published series where sicker patients may not be offered ECLS (14,20)
Prognostic Factors and Predictors of Mortality
Strong predictors of poor outcome include markedly elevated nonhemolyzed serum potassium (>10-12 mmol/L), which strongly associates with mortality, serves as a triage consideration in some ECLS protocols, reflects prolonged tissue hypoxia and cell death, though survivors with potassium exceeding 10 mmol/L have been reported, precluding absolute contraindication (1,2). Lower core temperature associates with higher mortality, with each degree below 28°C increasing risk and temperatures below 24°C historically associated with very poor outcomes, though survivors have been reported (2,4). Factors associated with better outcomes include younger age, previously healthy status, witnessed arrest or rapid discovery, rapid CPR initiation, short transport time to ECLS centers, icy water submersion versus environmental exposure, and ventricular fibrillation as presenting rhythm (1,2,22).
Neurological Outcomes
Hypothermia’s neuroprotective effects result from reduced cerebral metabolic rate, decreased oxygen consumption, potential neurological function preservation during prolonged arrest, and form the basis for therapeutic hypothermia post-cardiac arrest (1,22). Full neurological recovery remains possible even after prolonged cardiac arrest (>60 minutes in cold water), profound hypothermia (<24°C), and prolonged resuscitation, with case reports documenting complete recovery with return to baseline function (22).
Even in profound hypothermic cardiac arrest, patients can achieve full survival and neurological recovery due to hypothermia’s neuroprotective effects, particularly when rapid CPR and timely ECLS are provided.
Current evidence and guidelines
Major Guideline Recommendations
American Heart Association (AHA)/Advanced Cardiovascular Life Support (ACLS) key recommendations include gentle handling to prevent ventricular fibrillation, prevention of further heat loss, staged rewarming approach (passive → active external → active internal
→ extracorporeal), modified resuscitation algorithms
limiting defibrillation attempts (up to three shocks) with deferral of repeated shocks until core temperature exceeds 30°C, withholding or spacing resuscitation drugs when temperature remains below 30°C, continuing cardiopulmonary resuscitation during rewarming, administering warmed humidified oxygen, providing warmed intravenous fluids (central administration preferred), considering extracorporeal rewarming for cardiac arrest or hemodynamic instability, and continuing resuscitation until rewarmed consistent with the principle “no one is dead until they are warm and dead” (1). European Resuscitation Council (ERC) recommendations align with AHA guidance with variations including emphasis on early ECLS triage for severe cases, structured regional protocols for hypothermia management, consideration of mechanical CPR for prolonged transport, and specific temperature thresholds for treatment modifications (2). Wilderness Medical Society provides specific guidance for remote settings including field rewarming techniques when evacuation is delayed, decision algorithms for field versus evacuation, and practical considerations for resource-limited environments (23). International Commission for Mountain Emergency Medicine (ICAR MEDCOM) endorsed recommendations include temperature-based staging and triage, ECLS as preferred method for severe hypothermia with arrest, regional coordination for mountain rescue and hypothermia care, and specific protocols for avalanche victims (2). It is also of importance to mention Croatian national recommendations for diagnosis and treatment of accidental hypothermia in emergency medicine which present contribution to successful management of accidental hypothermia (24).
Accidental hypothermia, caused by environmental exposure, medical conditions, trauma, or drugs, is life-threatening and requires early recognition and careful management, especially in vulnerable populations.
Conclusion
Accidental hypothermia is most often caused by environmental exposure, but medical conditions, trauma, drugs, and social factors also increase risk. Submersion in cold water can rapidly induce hypothermia, sometimes with brain-protective effects. Mortality rates are significant but likely underreported. Medical conditions such as endocrine disorders, cardiovascular disease, and infections, especially in infants and the elderly, heighten vulnerability. Trauma-related hypothermia worsens outcomes due to its role in the “lethal triad.” Certain drugs and toxins further impair the body’s ability to regulate temperature. Older adults, infants, the homeless, and those with mental illness or substance use are particularly at risk. Iatrogenic hypothermia can occur during surgery or with unwarmed transfusions, and therapeutic hypothermia requires careful monitoring. Early recognition, prevention, and tailored management are essential to improve outcomes in hypothermic patients.
References
- European Resuscitation Council. Part 8: advanced challenges in resuscitation. Section 3: special challenges in ECC 3A: hypothermia. Resuscitation. 2000 Aug 23;46(1–3):267–271. doi:10.1016/s0300-9572(00)00288-4.
- Paal P, Gordon L, Strapazzon G, Brodmann Maeder M, Putzer G, Walpoth B et al. Accidental hypothermia—an update: The content of this review is endorsed by the International Commission for Mountain Emergency Medicine (ICAR MEDCOM). Scand J Trauma Resusc Emerg Med. 2016;24:111. doi:10.1186/S13049-016-0303-7.
- Maclean D. Emergency management of accidental hypothermia: a review. J R Soc Med. 1986;79(9):528–531. doi:10.1177/014107688607900909.
- Rischall ML, Rowland-Fisher A. Evidence-Based Management of Accidental Hypothermia in the Emergency Department. Emerg Med Pract. 2016;18(1):1–21. PMID: 26655247.
- McCullough LB, Arora S. Diagnosis and treatment of hypothermia. Am Fam Physician. 2004;70(12):2325–2332. PMID: 15617296.
- Jacobson E, Briggs S, Lundeby H, Gunderson E, Weingarten T. Accidental Hypothermia in the Upper Midwest: A Dual Case Report Comparison. J Case Rep Stud. 2016;4(2):208. doi:10.15744/2348-9820.4.208.
- Pirnes J, Nyländen J, Karjalainen TM, Sälkiä S, Ohtonen P, Hoikka M et al. Factors related to 30-day survival rate following accidental hypothermia – a retrospective single-center study from Northern Finland. Scand J Trauma Resusc Emerg Med. 2025 Nov 7;33(1):179. doi:10.1186/s13049-025-01491-3.
- Kosiński S, Darocha T, Gałązkowski R, Drwiła R. Accidental hypothermia in Poland – estimation of prevalence, diagnostic methods and treatment. Scand J Trauma Resusc Emerg Med. 2015;23:13. doi:10.1186/S13049-014-0086-7.
- Rasmussen JM, Cogbill TH, Borgert AJ, Pieracci FM, Haenel JB, Magnotti LJ et al. Epidemiology, management, and outcomes of accidental hypothermia: a multicenter study of regional care. Am Surg. 2021;87(3):458–464. doi:10.1177/0003134820984869.
- Perlman R, Callum J, Laflamme C, Tien H, Nascimento B, Beckett A et al. A recommended early goal-directed management guideline for the prevention of hypothermia-related transfusion, morbidity, and mortality in severely injured trauma patients. Crit Care. 2016 Apr 20;20(1):107. doi:10.1186/s13054-016-1271-z.
- Harten-Ash L, Hudson A. Hypothermia among trauma patients in the Emergency Department (ED): a review of documentation and management. Scand J Trauma Resusc Emerg Med. 2014;22(Suppl 1):P10. doi:10.1186/1757-7241-22-S1-P10.
- Demirer E, Ghattas C, Abdel Rahman H, Sayan M, Ulus T. Current Management of Hypothermia: From Theory to Application. Respir Case Rep. 2012;1(1):31–36. doi:10.5505/RESPIRCASE.2012.36844.
- Chivers K. Accidental hypothermia: pathophysiology, investigations and management. Emerg Nurse. 2022;30(6):18–24. doi:10.7748/en.2022.e2147.
- Prekker ME, Rischall M, Carlson MD, Koehler RC, Wick EC, Daya MR. Extracorporeal membrane oxygenation versus conventional rewarming for severe hypothermia in an urban emergency department. Acad Emerg Med. 2023;30(2):107–117. doi:10.1111/acem.14585.
- Maclean D. Emergency management of accidental hypothermia: a review. J R Soc Med. 1986;79(9):528–531. doi:10.1177/014107688607900909.
- Savioli G, Ceresa IF, Bavestrello Piccini G, Longhitano Y, Zanza C, Piccioni A et al. Hypothermia Beyond the Narrative Review—The Point of View of Emergency Physicians and Medico-Legal Considerations. J Pers Med. 2023;13(12):1690. doi:10.3390/jpm13121690.
- Lyon R, Robertson C, Clegg G. Therapeutic hypothermia in the emergency department following out-of-hospital cardiac arrest. Emerg Med J. 2010;27(6):418–423. doi:10.1136/EMJ.2009.089821.
- Lo YH, Ramgopal S, Hashikawa AN, Monuteaux MC, Neuman MI. Variability in emergency department management of hypothermic infants ≤90 days of age. Am J Emerg Med. 2022;60:90–95. doi:10.1016/j.ajem.2022.07.058.
- Chivers K. Accidental hypothermia: pathophysiology, investigations and management. Emerg Nurse. 2022;30(6):18–24. doi:10.7748/en.2022.e2147.
- Rasmussen JM, Cogbill TH, Borgert AJ, Pieracci FM, Haenel JB, Magnotti LJ et al. Epidemiology, management, and outcomes of accidental hypothermia: a multicenter study of regional care. Am Surg. 2021;87(3):458–464. doi:10.1177/0003134820984869.
- Adler DS, Bezerko M, Trueger NS, Lo AX. Foley Tubing as a Luer Adapter for Thoracic Lavage in Severe Hypothermia. J Emerg Med. 2025 Dec;79:502–506. doi:10.1016/j.jemermed.2025.09.025.
- Delvecchio K, Marinica AL, Williams C, Saavedra AC, Surani S. Complete Neurological Recovery after Severe Accidental Hypothermia: Two Cases and a Novel Algorithm Proposal. Am J Med Case Rep. 2019;7(6):119–123. doi:10.12691/AJMCR-7-6-2.
- Jacobson E, Briggs S, Lundeby H, Gunderson E, Weingarten T. Accidental Hypothermia in the Upper Midwest: A Dual Case Report Comparison. J Case Rep Stud. 2016;4(2):208. doi:10.15744/2348-9820.4.208.
- Majhen-Ujević R, Bošan-Kilibarda I, Brdar I, Olujić V, Ferri Certić I, Kajčić S et al. Preporuke za dijagnostiku i liječenje slučajnog pothlađivanja u hitnoj medicinskoj službi. Medicina Fluminensis. 2024;60(4):472–481. doi:10.21860/medflum2024_321531.