Introduction
The treatment of pain is a fundamental aspect of emergency medical care. Administration of analgesia by oral, intra-muscular and intravenous routes is so common as to barely merit comment, while infiltration of local anesthetics is similarly a daily part of patient care. While regional anesthesia has been a part of the emergency medicine specialist’s practice for decades, the introduction of ultrasound has expanded the scope and precision of regional anesthesia in the emergency department (1). Regional anesthesia is the unsung hero of emergency department analgesia: it allows powerful reduction of pain while sparing use of opioid analgesics that can complicate patient care in those at risk of respiratory and hemodynamic impairment, as well as those at risk of delirium (2).
Ultrasound guided nerve block of the hip can be successfully performed by emergency physicians.
One place where regional anesthesia has been consistently shown to improve patient pain and reduce the complications of opioid use is in the patient with an acute fractured hip.
(4). Regional anesthesia for hip fracture (referring here to both femoral neck and intertrochanteric femur fractures) began as femoral nerve blocks and landmark-based fascia iliaca nerve blocks to the ultrasound guided supra-inguinal fascia iliaca nerve block and, more recently, the pericapsular nerve group (PENG) block. This paper will review the PENG block, detailing its indications and correct performance, as well as complications that can arise while performing the block and how to successfully avoid them.
Methods
We began this narrative review with a literature search in PubMed and Google Scholar, using keywords ‘PENG Block,’‘pericapsular nerve group block,’‘regional anesthesia of the hip,’ ‘nerve block of the hip’ and related terms to identify relevant studies. The search was not intended to be exhaustive, but rather to identify the most current ideas on the performance of the PENG block, with the focus upon how the block is performed, its common complications and how to avoid these complications, and its efficacy.
Origins of the PENG Block
The pericapsular nerve group (PENG) block was first described in 2018 by Drs. Girón-Arango, Peng, Chin and their team. The technique was developed to reduce pain after total hip arthoplasties while minimizing nerve blockade to motor nerves to allow for early rehabilitation (3).
The PENG block is a novel method of providing anesthesia to the hip that is efficacious and easy to perform.
Indications
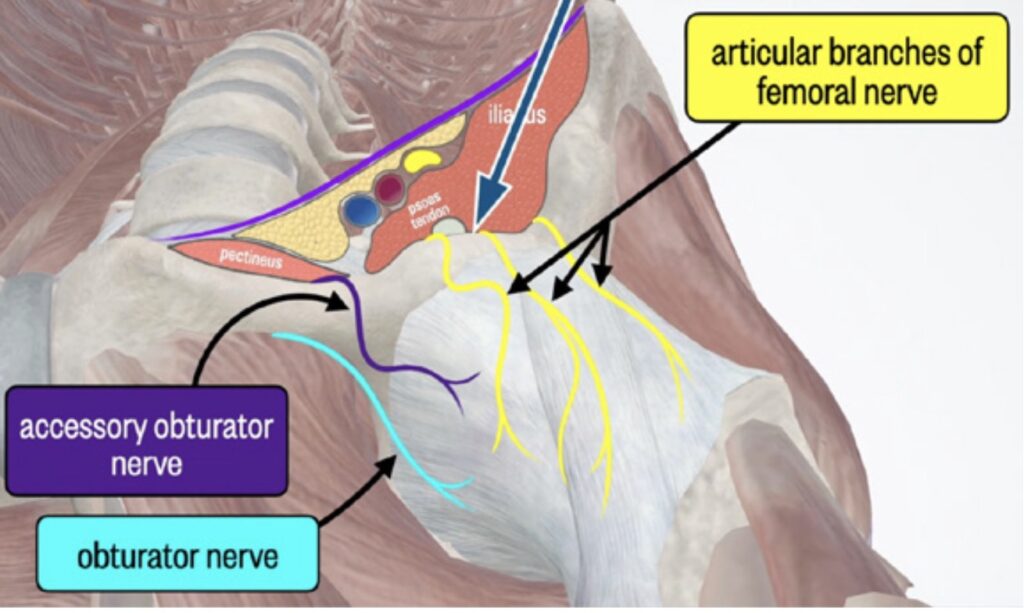
The PENG block provides anesthesia to anteromedial aspect of joint capsule of the hip. Because most sensory nerves for the hip run in the anterior aspect of the joint capsule, it will effectively capture these nerves (5). There is also some spread of anesthesia beyond the anteromedial joint capsule, which allows blockade of nerves innervating surrounding soft tissues (iliopsoas muscle, etc) (3, 6-7). Practitioners should be aware that administration of high volumes of anesthetic can result in femoral nerve blockade, potentially causing quadriceps weakness (8).
The PENG block provides excellent anesthesia for acetabular fractures and femoral neck fractures. It can provide anesthesia for intertrochanteric or subtrochanteric fractures, but the effect is not always as consistent. In such cases, consideration should be given to performing a suprainguinal fascia iliaca block, either as the primary regional anesthesia technique or as an adjunct if the PENG block fails to achieve adequate pain control.
How to Perform the PENG Block
- Obtain consent and gather materials. You will need:
Required equipment includes topical local anesthetic (1% lidocaine), a long-acting local anesthetic such as ropivacaine or bupivacaine, sterile saline for flushing, a 10-mL syringe for local injections, and a 60-mL syringe for the plane block. Additional supplies include IV extension tubing approximately 10 cm in length, an 18-gauge needle for drawing up anesthetic agents, a 25-gauge needle for skin anesthesia, and a 21-gauge nerve block needle (or a non-cutting spinal needle) for block performance. When possible, an 80-mm needle should be selected to ensure adequate length, particularly in patients with a larger body habitus. Ultrasound equipment should be available, including an ultrasound machine and a sterile ultrasound probe cover. Skin preparation should be performed using chlorhexidine, and sterile gloves should be worn throughout the procedure.
- Place the patient on a cardiac monitor to ensure the team will be altered to the accidental intravascular administration of high dose local anesthetic.
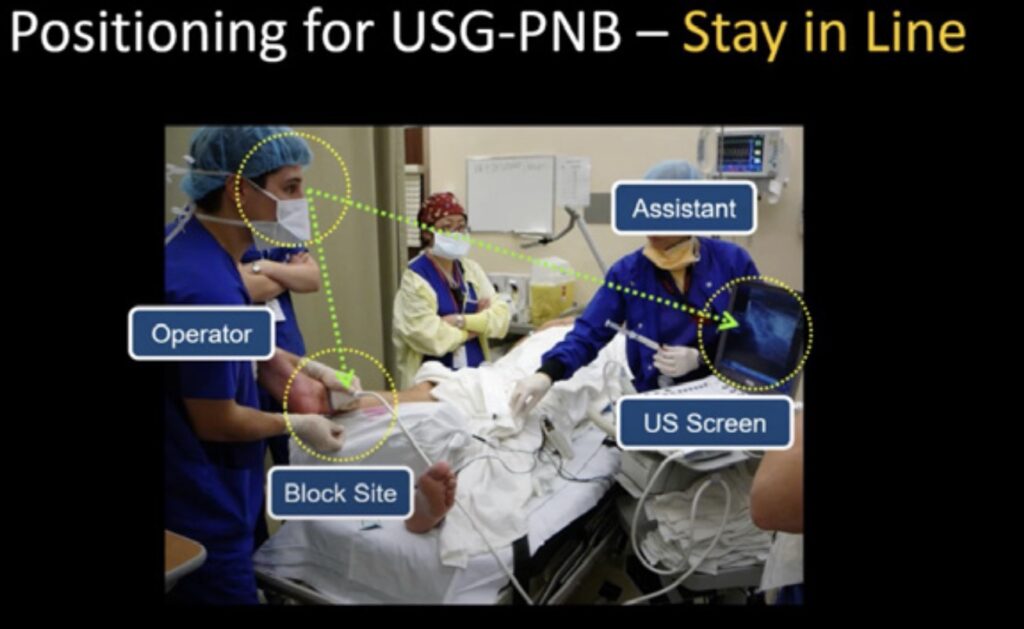
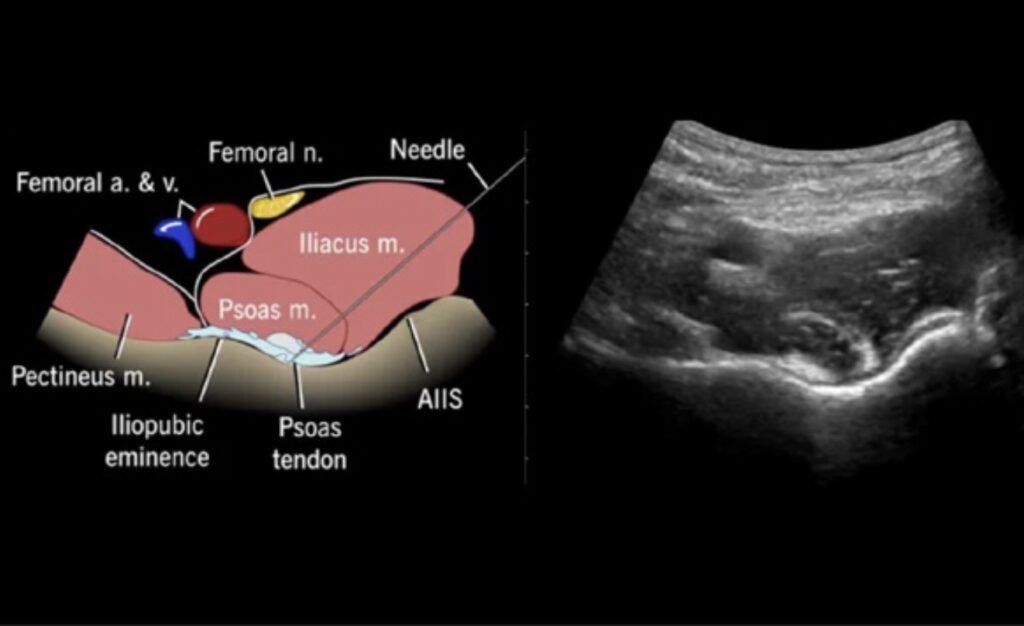
- Orient the ultrasound and patient to facilitate performance of the block (figure 1).
- Complete patient skin cleaning and preparation with chlorhexidine (preferred) and/or provodone/iodine.
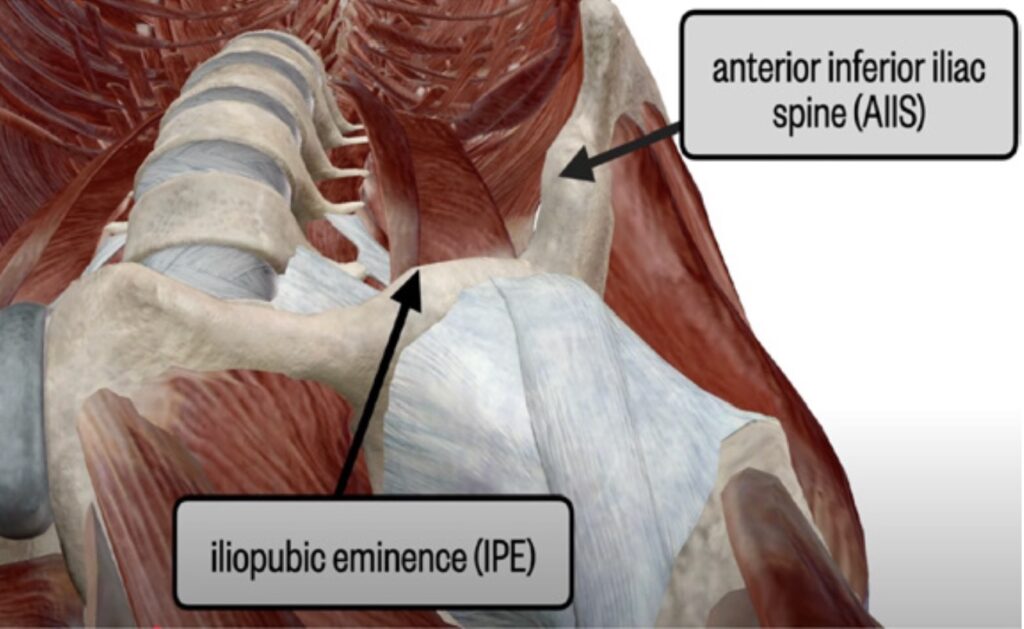
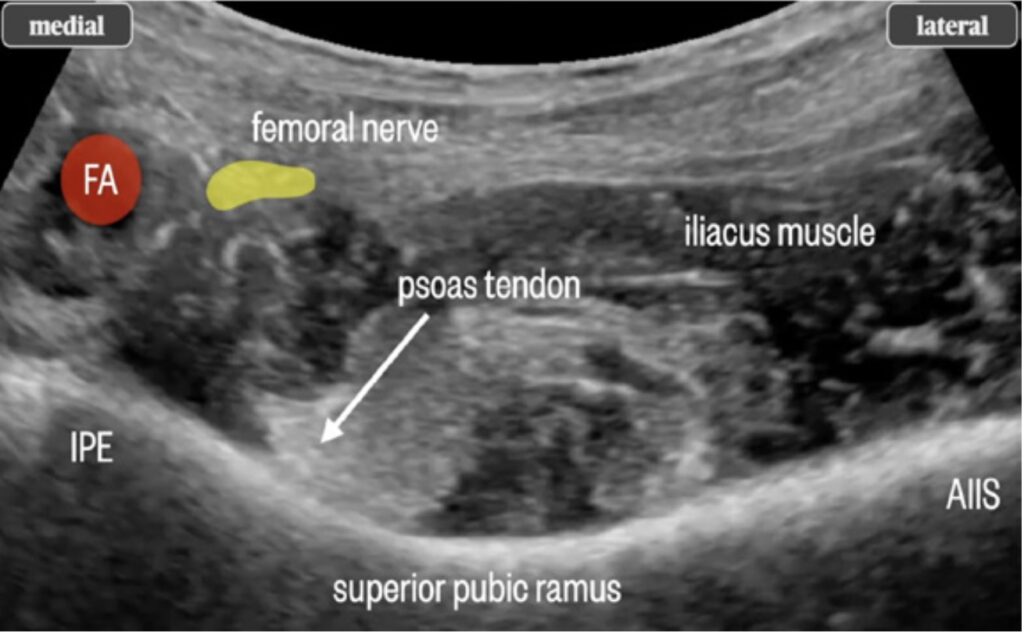
- Using either a linear or curved transducer, place the ultrasound probe over the anterior superior iliac spine, then move the probe medially to find the anterior inferior iliac spine and psoas muscle. For larger patients, the curvilinear probe often affords better visualization.
- Administer skin anesthetic. Take care to avoid the lateral femoral cutaneous nerve. Attach the 60ml syringe to the extension tubing and the extension tubing to the needle to be used for performance of the nerve block. This allows the operator to keep the needle in position while an assistant delivers the anesthetic with the 60ml syringe.
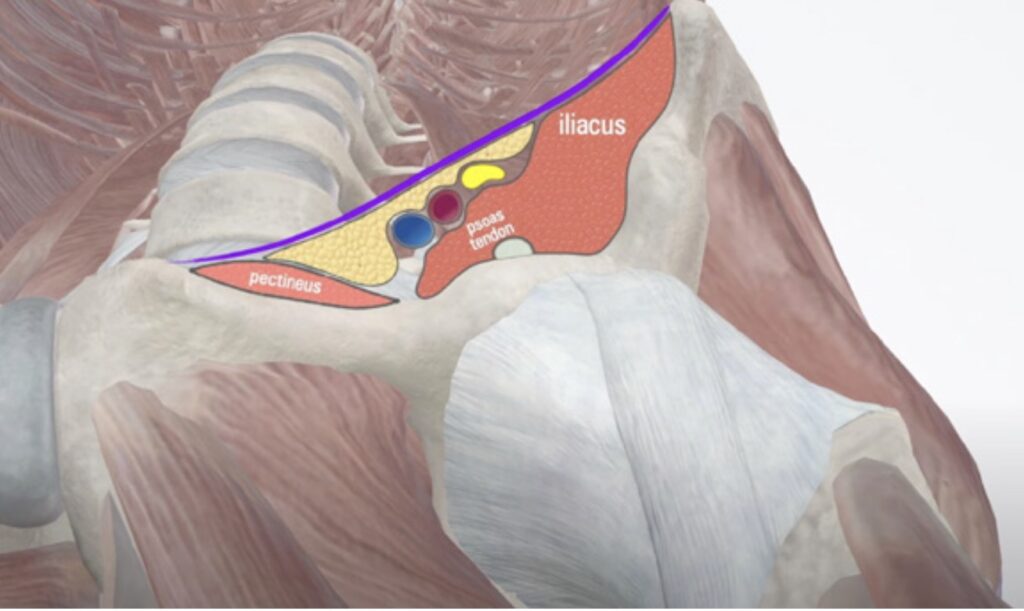
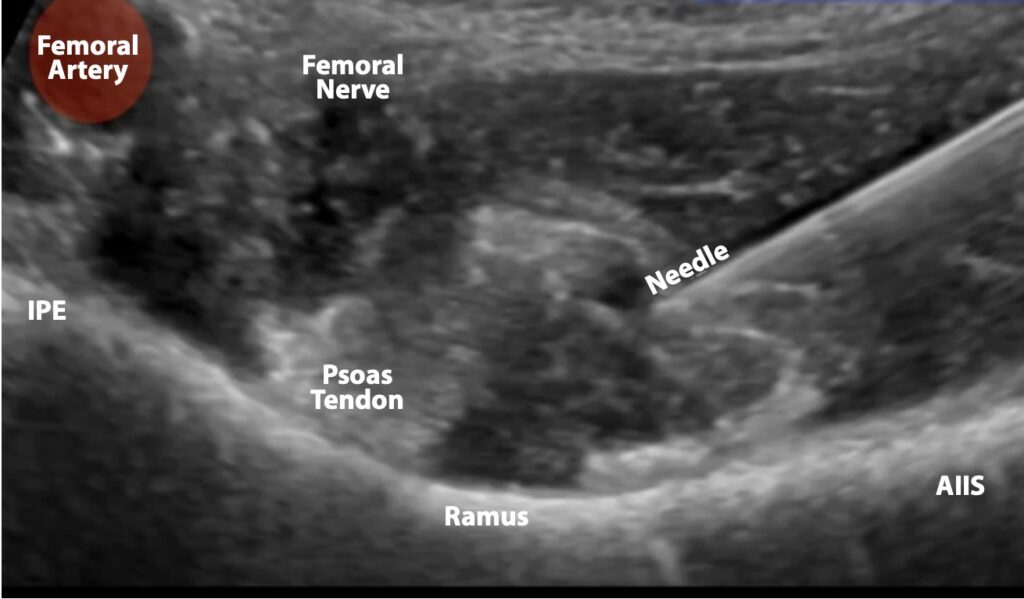
- Advance the needle under direct visualization to the psoas muscle. Use an in-plane approach, moving from lateral to medial until contact with the ilium is made under the psoas tendon (figures 3,4,5).
- Once on the fascia investing the bone beneath the psoas tendon, spin the needle to help ensure the needle cuts below fascia.
- Administer a test saline injection of 0.5ml normal saline to ensure the needle is not in muscle or tendon.
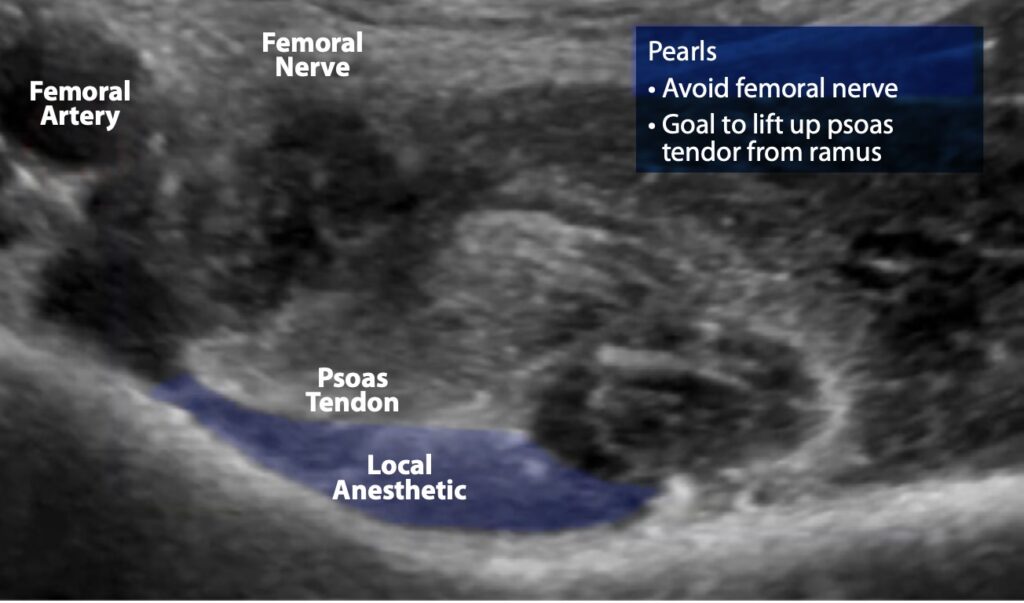
- Now administer 15-20 ml of dilute local anesthetic. Highly concentrated anesthetic is not needed for the PENG block because the nerves are small. No more than 20ml is required for successful block (larger volumes of anesthetic increases the spread of anesthetic and the consequent risk of lumbar plexus blockade). Correct administration of anesthetic will cause a lift of the iliopsoas tendon (figures 5,6,7).
Complications and How to Avoid Them.
When performed with care and under direct ultrasound guidance, the risk of complications with the PENG block is low. There are, however, several complications the astute operator will look out for (9).
Complication number one: Accidental blockade of the femoral nerve with resulting quad weakness. As noted above, femoral nerve blockade is usually a consequence of overzealous administration of local anesthetic during the block (i.e. the operator administers too much volume). This will cause quad and hip weakness, which is not a problem in the emergency department, but can lead to difficulty with rehabilitation after surgical repair if the block is performed immediately prior to surgery.
The most important complication to avoid is femoral nerve blockade, which occurs when excessive local anesthetic is administered.
Complication number two: Inadvertent intravascular injection and local anesthetic toxicity. When the block is performed correctly under ultrasound guidance, the femoral vasculature is distant from the block site and the consequent risk of this complication is low. It is important to note that the toxicity is higher with bupivacaine than with lidocaine.
Complication number three: Inability to injection anesthetic due to high resistance. While not a true complication, high resistance to injection can render the PENG block difficult to execute. This occurs when the needle is not in the right location or the fascia has not been penetrated. There should be some resistance to injection, but if resistance is very high, ask yourself: are you in the right place?
Complication number four: After administration of the block, the anesthetic moves out of place. This complication is more common with other nerve blocks (for example, the fascia iliaca nerve block), it can occur if the anesthetic is administered in the wrong location, or if too much anesthetic is administered.
Complication number five: Allergic reaction to local anesthetic. Allergic reactions to local anesthetics are known to occur, and the mindful operator should watch for their occurrence, even if they are uncommon.
Discussion
The PENG block is a useful tool for emergency medicine specialists trying to treat the pain after hip fracture. We believe it is straightforward to learn, and straightforward to perform. While perhaps not the less effective for some hip fractures (intertrochanteric fractures), it has the has the benefit of analgesia with less motor nerve paralysis, allowing for more accurate assessment by orthopedic surgery prior to surgical repair.
Acknowledgements
This author acknowledges his deep debt to the work of Dr. Ki Jinn Chin of the University of Toronto, for his pioneering work in regional anesthesia. He is a peerless educator whose brilliance and generosity cannot be overstated.
References
-
Herring AA.
Bringing Ultrasound-guided Regional Anesthesia to Emergency Medicine.
AEM Educ Train. 2017;1(2):165–168.
doi:10.1002/aet2.10027.
-
Ritcey B, Pageau P, Woo MY, Perry JJ.
Regional Nerve Blocks For Hip and Femoral Neck Fractures in the Emergency Department: A Systematic Review.
CJEM. 2016;18(1):37–47.
doi:10.1017/cem.2015.75.
-
Girón-Arango L, Peng PWH, Chin KJ, Brull R, Perlas A.
Pericapsular Nerve Group (PENG) Block for Hip Fracture.
Reg Anesth Pain Med. 2018 Nov;43(8):859–863.
doi:10.1097/AAP.0000000000000847. PMID:30063657.
-
Luftig J, Dreyfuss A, Mantuani D, Howell K, White A, Nagdev A.
A new frontier in pelvic fracture pain control in the ED: Successful use of the pericapsular nerve group (PENG) block.
Am J Emerg Med. 2020 Dec;38(12):2761.e5–2761.e9.
doi:10.1016/j.ajem.2020.05.085.
-
Akkaya T, Comert A, Kendir S, Acar HI, Gumus H, Tekdemir I, Elhan A.
Detailed anatomy of accessory obturator nerve blockade.
Minerva Anestesiol. 2008 Apr;74(4):119–122.
-
Short AJ, Barnett JJG, Gofeld M, Baig E, Lam K, Agur AMR, Peng PWH.
Anatomic Study of Innervation of the Anterior Hip Capsule: Implication for Image-Guided Intervention.
Reg Anesth Pain Med. 2018 Feb;43(2):186–192.
doi:10.1097/AAP.0000000000000701.
-
Tran J, Agur A, Peng P.
Is pericapsular nerve group (PENG) block a true pericapsular block?
Reg Anesth Pain Med. 2019;44(2):257–257.
doi:10.1136/rapm-2018-100278.
-
Yu HC, Moser JJ, Chu AY, Montgomery SH, Brown N, Endersby RVW.
Inadvertent quadriceps weakness following the pericapsular nerve group (PENG) block.
Reg Anesth Pain Med. 2019 May;44(5):611–613.
doi:10.1136/rapm-2018-100354.
-
Mysore K, Sancheti SA, Howells SR, Ballah EE, Sutton JL, Uppal V.
Postoperative analgesia with pericapsular nerve group (PENG) block for primary total hip arthroplasty: a retrospective study.
Can J Anaesth. 2020 Nov;67(11):1673–1674.
doi:10.1007/s12630-020-01751-z.