Introduction
Foley`s catheterization is one of the common and usually safe procedures done in hospital and in community as well. However it also carries risk of some common complications like infection, urethral trauma, bleeding, bladder spasm, leakage, irritation or pain at urethral meatus but also carries risk of some very rare and serious complications like rupture of ureter (1). We report a similar case of ureteric rupture following Foley`s catheter balloon inflation in community by general physician and patient was initially managed at emergency department and then referred to a urology tertiary referral centre.
Ureteric rupture is a rare but serious complication of Foley’s catheterization that can occur due to inadvertent intra-ureteric balloon inflation and should be suspected in patients presenting with acute abdominal pain and sepsis after the procedure.
Case report
In June 2023, a male in his 70’s was referred from general physician to our emergency department with severe lower abdominal pain following attempt of Foley`s catheterization.
General physician attempted Foley`s catheterization with a 16 Fr Foley`s catheter due to recurrent urinary incontinence and deranged renal functions of the patient but unfortunately patient developed sudden severe lower abdominal pain with a pain score of 10/10. The general physician stopped and repositioned the catheter, which lead to frank haematuria. After that general physician attempted with 14Fr size Foley`s catheter but it started bypassing when he tried to flush it. Therefore he removed the catheter. The patient was then referred to our Emergency department.
On arrival to Emergency department, patient was complaining of severe lower abdominal pain. On examination, he was apyrexial, tachycardiac 109 per minute and tachypnoeic 24 per minute. His lower abdomen was tender on palpation. His lactate was 3.99 mol/L, white blood cells count of 17.3 and C reactive protein of 31. A bed side urinary bladder ultrasound scan revealed 10 ml volume. He was commenced on sepsis six bundle. His case was discussed with Urology department in a tertiary referral centre. They advised to do a CT Urogram with query of bladder perforation. CT Urogram with contrast revealed left ureter rupture with contrast extravasation and retroperitoneal haematoma (figure 1).
Early imaging with CT urogram enables prompt diagnosis of ureteric rupture allowing timely referral and definitive intervention.
The patient was urgently transferred to urology team for further management. The Patient was admitted in ICU in the tertiary referral centre and had continuous bladder irrigation commenced. It was planned for Interventional radiology insertion of a left percutaneous nephrostomy but it was delayed because patient was administered edoxaban 1 day previously. The following day, the Interventional Radiology team successfully performed a left percutaneous nephrostomy and also placed an anterograde stent. Patient’s nephrostomy was removed by interventional radiology after 7 days while the anterograde stent was left in place. Patient was discharged from the hospital with a follow up plan as an outpatient in 10 weeks. Patient total length of stay in hospital was 2 weeks. After 4 months, cystoscopy was done along with
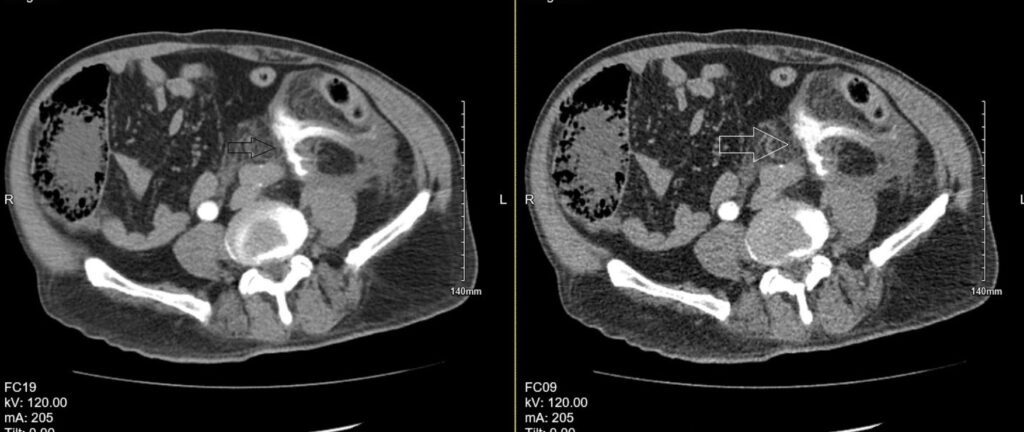
Figure 1. Contrast-enhanced CT demonstrating rupture of the left ureter with active contrast extravasation and associated retroperitoneal haematoma.
JJ stent removal as a day case and patient was discharged on same day with no further urology follow up plan. Informed consent for publication of this case was obtained.
Discussion
Ureteric rupture following Foley`s catheterization is rare and 8 cases have been reported in the literature in the past. This complication happens when the catheter accidently goes into the ureter and then the balloon is inflated inside the ureter, which might lead to rupture or tearing of ureter. The key warning sign is severe abdominal pain which starts after inflation of catheter balloon, especially if there is little or no urine draining through the catheter.
A literature review (2) published in 2024 identified 48 patients across 39 published case reports of inadvertent ureteric catheterization. Among these the most frequent complications of inadvertent ureteric catheterisation were acute pyelonephritis (35%), acute kidney injury (27%), urosepsis (21%) and ureteric rupture (17%). In our case, the patient developed both ureteric rupture and urosepsis, which are among the more severe reported outcomes. The most important way to prevent it is to confirm urine flow before inflating the balloon.
Prevention of ureteric injury relies on confirming free urine flow before balloon inflation and immediate cessation of the procedure if severe pain occurs, followed by urgent urological assessment and imaging.
If the patient experiences sudden, severe abdominal pain during balloon insertion or inflation, the balloon should be deflated immediately, the catheter removed, and further assessment should include prompt imaging and consultation with the urology team.
References
- Singh NP, Eardley I. An uncommon complication of urethral catheterization. Br J Urol. 1996 Feb;77(2):316-7. doi: 10.1046/j.1464-410x.1996.91532.x.
- Li JJ, Au CF. Inappropriate placement of urinary catheters into the ureter: A case report and literature review. Medicine (Baltimore). 2024;103(15):e37623. doi: 10.1097/MD.0000000000037623.
